
| TABLE 1 Childhood Thyroid Cancer Near Chernobyl (before and after the 1986 accident) |
|||||||
| 1981-1985 | 1986-1990 | 1991-1994 | |||||
|---|---|---|---|---|---|---|---|
| No. of Cases |
Rate* | No. of | Rate* | No. of Cases |
Rate* | Thyroid Dose Estimate | |
| Gomel region, Belarus | 1 | 0.5 | 21 | 10.5 | 143 | 96.4 | 15 to 570 rad |
| Northern Ukraine | 1 | 0.1 | 21 | 2.0 | 97 | 11.5 | 5 to 200 rad |
| Bryansk and Kaluga regions, Russia | 0 | 0 | 3 | 1.2 | 20 | 10.0 | 6 to 180 rad |
*number of thyroid cancers per million people [adapted from Stsjazhko et al. 1995]
Medical Exposures to Iodine-131
Much of what is currently known about the health effects of iodine-131 comes from studies of the medical uses of iodine-131. One group of people exposed to iodine-131 received a one-time high dose (thousands of rad) to treat hyperthyroidism (an overactive thyroid gland). Another group received a one-time low dose (50-100 rad) of iodine-131 for tests to diagnose thyroid disease. Studies of these two groups of people do not show any link between iodine-131 and thyroid cancer.
However, the length of time people were studied varied. The longest study followed people an average of 20 years. Investigators believe that the latent period for thyroid cancer can range from 5 to more than 40 years. They believe that the very high doses of iodine-131 used to treat people with hyperthyroidism result in killing off cells so that cancer cannot develop.
External Gamma and X-ray Radiation of the Thyroid
While there is not conclusive evidence linking iodine-131 and thyroid cancer, there is a link between thyroid cancer and exposure to X-rays and gamma radiation. Studies of people who received X-ray treatments of the head and neck show that X-rays can cause thyroid cancer. Thyroid cancer was the first solid tumor to show an increased rate in Japanese atomic bomb survivors who were exposed to gamma radiation.
Parathyroid Disease
Parathyroid glands help maintain the level of calcium in the body and are located around the thyroid. Studies of people receiving X-ray treatments to the head and neck have demonstrated a higher rate of hyperparathyroidism than expected. Further, those people who had hyperparathyroidism and a history of radiation treatments also had a greater frequency of thyroid disease than those who had hyperparathyroidism but did not have radiation treatments[12]. Radioactive iodine in the thyroid exposes the parathyroid and may cause tumors in the parathyroid glands. HTDS is investigating whether hyperparathyroidism is increased among people exposed to Hanford's radioactive releases.
Other Radiation Health Effects
Although cancer is the most studied of all radiation health effects, exposure to radiation can harm the human body in other ways. The following are brief summaries of some other radiation health effects. Publications are available from the Network on some of these health effects.
Immune System
Studies have shown that radiation exposure can weaken the immune system [13]. While there are no studies concerning Hanford and autoimmune diseases, some Hanford-area residents are concerned that their exposure to radioactive materials has triggered such diseases. They believe that there are a higher-than-usual number of autoimmune disease cases among those who were exposed.
Genetic Effects and Birth Defects
Genetic effects of radiation exposure occur when radiation damage to a parent's DNA code is transmitted to a child. Genetic effects caused by radiation fall into two categories: (1) effects that appear in the children of an exposed parent and (2) effects that appear in later generations. Birth defects can arise spontaneously or through harm to normal developmental processes by radiation or by other toxic exposures. For more information about possible genetic health effects, see Module 8.
Nervous System
Module 9 describes the possible nervous system diseases related to high-dose and low-dose radiation exposure. Past studies on radiation effects involving the nervous system are summarized.
Other Effects on the Lives of Those Who Were Exposed
The secrecy surrounding the Hanford releases, the involuntary nature of the exposure and the lack of information about radiation health effects have left some people understandably frustrated, mistrustful, and angry. Many people report feeling that the emotional and economic toll has been great. This is especially true for those who have thyroid diseases and other illnesses and whose family members, friends, and neighbors are ill or have died.
Conclusion
About 2 million people were exposed to environmental releases of radiation from Hanford's nuclear weapons operations from 1944 to 1972. Radiation can cause health effects, including cancer and thyroid disease. It is not known now what the health impact has been from the Hanford releases. More information will be available when the HTDS is completed in late 1998. However, given the uncertainties, the full impact of Hanford's releases will probably never be known.
NOTES
1. National Research Council (BEIR V). Health Effects of Exposure to Low Levels of Ionizing Radiation. National Academy Press, 1990. BEIR V was a committee of 17 scientists from the National Academy of Sciences. The chair of BEIR V was Arthur C. Upton.
2. BEIR V, p. 162.
3. T. Straume, et al. "Neutron Discrepancies in the DS86 Hiroshima Dosimetry System." Health Physics, October 1992, Vol. 63, No. 4, pp. 421-426. In 1992, Straume was with Lawrence Livermore National Laboratory. His colleagues were from SAIC in San Diego, the University of Rochester (N.Y.) and Hiroshima University.
4. J.W. Gofman. Radiation-Induced Cancer from Low-Dose Exposure: An Independent Analysis. Committee for Nuclear Responsibility, 1990, chapter 25, p. 15. Gofman is Professor Emeritus of Molecular and Cellular Biology at the University of California, Berkeley.
5. R.H. Nussbaum and Wolfgang K�hnlein. "Inconsistencies and Open Questions Regarding Low-Dose Health Effects of Ionizing Radiation." Environmental Health Perspectives, Vol. 102, No. 8, August 1994, pp. 656-667. Nussbaum is Professor Emeritus of Physics and Environmental Sciences at Portland (OR) State University. K�hnlein is professor and director of the Institute for Radiation Biology at the University of M�nster in Germany. See also "Health Consequences of Exposures to Ionizing Radiation from External and Internal Sources: Challenges to Radiation Protection Standards and Biomedical Research," Medicine and Global Survival, Vol. 2, No. 4, December 1995, pp. 198-213.
6. R.A. Kerber, et al. "A Cohort Study of Thyroid Disease in Relation to Fallout from Nuclear Weapons Testing." Journal of the American Medical Association, Vol. 270, No. 17, November 3, 1993, p. 2082.
7. V.A. Stsjazhko, et al. "Childhood Thyroid Cancer Since Accident at Chernobyl" (letter). British Medical Journal, Vol. 310, March 25, 1995, p. 801.
8. Table is adapted from V.A. Stsjazhko, et al. "Childhood Thyroid Cancer Since Accident at Chernobyl" (letter). British Medical Journal, Vol. 310, March 25, 1995, p. 801.
9. Technical Steering Panel of the Hanford Environmental Dose Reconstruction Project. Representative Hanford Radiation Dose Estimates, Revision 1. April 21, 1994, p. 2.
10. M. Balter. "Children Become the First Victims of Fallout." Science, Vol. 272, April 19, 1996, p. 359.
11. E. Ron, J. Lubin, and A.B. Schneider. "Thyroid Cancer Incidence." Nature, Vol. 360, November 12, 1992, p. 113. Ron and Lubin are with the Epidemiology and Biostatistics Program at the National Cancer Institute. Schneider is with Humana and Michael Reese hospitals at the University of Illinois.
12. A. Katz and G.D. Braunstein. "Clinical, Biochemical, and Pathologic Features of Radiation-Associated Hyperpara-thyroidism." Archives of Internal Medicine, Vol. 143, January 1983, pp. 79-82. [Back to Text]
13. M.M. Kaplan, et al. "Thyroid, Parathyroid, and Salivary Gland Evaluations in Patients Exposed to Multiple Fluoroscopic Examinations during Tuberculosis Therapy: A Pilot Study." Journal of Clinical Endocrinology and Metabolism, Vol. 66 (2), 1988, pp. 376-382.
A.D. Sadovnick and G.C. Ebers. "Epidemiology of Multiple Sclerosis: A Critical Overview." Le Journal Canadien des Sciences Neurologiques, Vol 20, 1990, p. 21.
D.R. Wynn, M. Rodriguez, W.M. O'Fallon, and L.T. Kurland. "A Reappraisal of the Epidemiology of Multiple Sclerosis in Olmsted County, Minnesota." Neurology, Vol. 10, 1990, pp. 780-786. [Back to Text]
The Hanford Thyroid Disease Study, authorized by an act of Congress in 1988, is funded by the Centers for Disease Control and Prevention and is being conducted by the Fred Hutchinson Cancer Research Center in Seattle, Washington. The primary purpose of this epidemiologic study is to determine whether thyroid disease is increased among persons exposed to the releases of radioactive iodine from Hanford between 1944 and 1957. The Study will be completed in late 1998.
* The HEDR Project was formed in 1987 to estimate radiation doses the public may have received as a result of releases of radioactive materials from the Hanford Site. The Project was initially funded by the U.S. Department of Energy (DOE) and later funded by the U.S. Centers for Disease Control and Prevention (CDC).
References
For further reading about Hanford:
Atomic Harvest: Hanford and the Lethal Toll of America's Nuclear Arsenal by Michael D'Antonio (Crown Pub. 1993)
The Dragon's Tail: Radiation Safety in the Manhattan Project, 1942-1946 by Barton C. Hacker (University of California 1987)
On the Home Front: The Cold War Legacy of the Hanford Nuclear Site by Michele Stenehjem Gerber (University of Nebraska 1992)
Sordid Sorcery: The History of Hanford's Deception by the Hanford Education Action League (HEAL 1992).
Many callers to the Hanford Health Information Lines have questions and concerns about the release of plutonium and other radioactive materials from Hanford. Some downwinders have health problems and believe that they are, or might be, related to Hanford. The personal perspectives within this monograph are offered to help readers understand these experiences and concerns.
When I arrived in Richland in 1954, I was healthy, happy, full of energy, and a bride of two weeks. It wasn't long before I began having horrific migraines, and unexplained attacks of vomiting and diarrhea that sent me to the hospital because I was dehydrated. Tests could not explain my symptoms--yet they persisted. I was weak to the point of exhaustion. And I lost an alarming amount of weight.
"Within a few years it became impossible for me to participate in family and social events. More often than not, I stayed home and on more than one occasion, my husband and children went on vacation trips without me. Two of my pregnancies ended in miscarriages. By my early 30s, I was a semi-invalid. I was diagnosed with endometriosis. When I was 35, I was rushed to the hospital unconscious and hemorrhaging. An emergency hysterectomy saved my life. Seven years ago, I was diagnosed with fibromyalgia. Was it connected to living there (near Hanford)? The doctors didn't connect it--yet?
"Both of our children were born with immune dysfunctions. A simple cold was an alarming matter. They were often anemic and our pediatrician tested them for leukemia. Both had skin cancer. My adult daughter has endometriosis. Connected? I wonder. . . Without warning, my husband was diagnosed with prostate cancer. It had already metatasized to his kidney, then to his liver. He died in 1990. His question was, "Are our medical problems because we lived in Richland for 25 years?" It weighs heavily upon my heart. Is there a connection? Studies and medical monitoring may one day answer his question. We greatly miss his loving presence in our lives."
Name withheld by request
MODULE 3
The Release of Radioactive Material From Hanford: 1944-1972
OBJECTIVES
After studying this module, the reader will be able to
* provide to their patients a brief history of the releases of radioactive materials from Hanford
* identify some of the specific radionuclides that may have affected public health
* describe the project responsible for estimating doses from the releases of radioactive materials from Hanford
History
The United States government chose a location in south central Washington state in 1943 for the Hanford Nuclear Reservation- now known as the Hanford Site. The government moved area residents in order to build plants for making plutonium at Hanford.
Few people knew before 1945 why Hanford was built. Hanford workers and area residents learned that Hanford made plutonium when the United States dropped an atomic bomb on Hiroshima, Japan. Hanford plutonium was used in the bomb that was dropped on Nagasaki, Japan, and in the first atomic bomb tested in New Mexico.
Hanford began making plutonium in September 1944, and released radioactive materials into the air, water, and soil for more than forty years. However, most of the public and some of the Hanford workers did not know about these releases until 1986 when the United States Department of Energy, in response to public pressure, released 19,000 pages of documents to the public. These documents showed that planned and unplanned releases of radioactive materials from Hanford contaminated the air, the Columbia River, and the soil. The information in these documents led to the formation of the Hanford Environmental Dose Reconstruction Project (HEDR). [*] Citizen activists played an important role in the release of those and other Hanford documents to the public.
Many citizen groups opposed bringing nuclear waste to Hanford in the early 1980s. One group, the Hanford Education Action League (HEAL) formed in 1984, raised numerous questions about the past and present safety of Hanford. HEAL, along with other groups such as Physicians for Social Responsibility (PSR) and Hanford downwinders, pressed the U.S. Department of Energy for proof of Hanford's safety.
One month before the U.S. Department of Energy's release of the Hanford documents, HEAL, the Environmental Policy Institute in Washington, D.C., and several Northwest groups filed a Freedom of Information Act request for Hanford documents. This request resulted in a second release of documents.
HEDR has estimated the radiation doses the public may have received from Hanford from 1944 to 1992. According to HEDR's estimates, about 2 million people were exposed either through the air or the Columbia River.
By analyzing the 19,000 pages and other historical documents and by using computers, HEDR estimated how much radiation Hanford released and how much people were exposed to based on where they lived and what they ate and drank. For most of those exposed, the greatest part of their total dose came from drinking milk and eating food that was contaminated with radioactive materials from Hanford. For certain people, such as Native Americans, the largest contributor to dose was probably eating contaminated fish.
Air Releases
Most of Hanford's air releases came from the chemical process used to separate plutonium and uranium from fuel rods. Some of the air releases came from the nuclear reactors. The major radioactive releases occurred between 1944 and 1957. The largest ones were from December 1944 through 1947 when there were no filters on the stacks of the separations plants. Radioactive materials in the form of gases, vapors, and particles went up the stacks.
Hanford produced hundreds of radioactive substances. Most had no effect on public health because they were released in small amounts, became non-radioactive quickly, or resulted in little public exposure. HEDR estimates that iodine-131 was the major contributor to dose from the releases into the air. The project is also estimating doses from other radioactive material: ruthenium-103, ruthenium-106, strontium-90, plutonium-239, and cerium-144.
HEDR is re-evaluating early estimates of the amount of air releases from Hanford. In October 1992, HEDR announced new estimates that Hanford released 685,000 curies of radioactive iodine-131 between 1944 and 1947. This amount is based on information found in the U.S. Department of Energy documents made public in recent years.
In January 1994, HEDR presented a new estimate for the amount of iodine-131 which Hanford released between 1948 and 1957. The total estimate for these years was 52,060 curies. Also included in the information offered by HEDR were estimates of the amounts of iodine-131 and other radioactive material Hanford released into the air from 1944 to 1972. These figures are shown in Table 1 below.
HEDR is continuing to study the ruthenium and plutonium releases because some of the radiation released to the air was in the form of particles. Module 10 presents the current data and discusses the possible health effects of plutonium, strontium, cerium, and ruthenium. There are documents that describe how particles from inside the stacks of two Hanford plants collected ruthenium and plutonium. Some went beyond the Hanford Site when the particles broke off and were carried out the stacks. Estimates of the amounts of particles released and the doses received are not yet completed. HEDR plans to complete these estimates by the end of 1997 (see Module 10).
Iodine-131 remains the focus of HEDRs work because of the large amount released. The ways in which people were exposed to iodine-131 include eating contaminated fruits and vegetables, breathing contaminated air, and drinking contaminated milk.
Once in the body, iodine-131 concentrates in the thyroid gland. The most likely health effect of this exposure is thyroid disease. This effect is the subject of the Hanford Thyroid Disease Study (HTDS)[+] being conducted by the Fred Hutchinson Cancer Research Center in Seattle, Washington. HTDS is being conducted for the Centers for Disease Control and Prevention.
Columbia River Contamination
The first eight nuclear reactors at Hanford used large amounts of Columbia River water to cool the reactor cores. The water went through the reactors once before being returned to the Columbia River, even though the water contained radioactive materials. Radioactive materials that built-up inside the reactors were also regularly flushed loose and entered the Columbia River.
These eight reactors were operating at highest power between the late-1950s and mid-1960s. Contamination of the Columbia River was greatest during this time. The last of the eight reactors was shut down in January 1971.
HEDR now estimates that five radioactive substances account for most of the dose received from exposure to the Columbia River. They are arsenic-76, neptunium-239, phosphorus-32, sodium-24, and zinc-65 (Table 2).
People received exposure from the Columbia River by: eating contaminated fish and seafood; drinking contaminated water; swimming in or boating on the Columbia River; standing along the river shoreline or on a lawn irrigated with river water; and breathing dust blowing off exposed beaches or land irrigated with river water. Eating fish and seafood and drinking water were the main ways people were exposed to radiation from Hanford's reactors. Module 11 discusses the releases to and effects on the Columbia River. See Module 11: Radionuclides in the Columbia River.
Soil Contamination
The separations plants at Hanford required large amounts of water. Millions of gallons of highly radioactive waste from these plants are currently stored in tanks at Hanford. Billions of gallons of less radioactive water, which were put into trenches and surface ponds, seeped into the ground. Some radioactive materials traveled through the soil and entered the groundwater. Radioactive wastes were sent directly into the groundwater through "injection wells" or shafts dug into the soil.
Tritium is most commonly found in the groundwater at Hanford. Ruthenium-106, technetium-99, and iodine-129 are three of the other radioactive materials commonly found in Hanford's groundwater. Some radioactive substances still remain in the soil. HEDR believes there was little human contact with the contaminated groundwater in the past. If groundwater contamination from Hanford migrates under the Columbia River and contaminates water wells on the other side of the river in the future, this might pose a danger to the public.
NOTES
* The HEDR Project was formed in 1987 to estimate radiation doses the public may have received as a result of releases of radioactive materials from the Hanford Site. The Project was initially funded by the U.S. Department of Energy (DOE) and later funded by the U.S. Centers for Disease Control and Prevention (CDC).
+ The Hanford Thyroid Disease Study, authorized by an act of Congress in 1988, is funded by the Centers for Disease Control and Prevention and is being conducted by the Fred Hutchinson Cancer Research Center in Seattle, Washington. The primary purpose of this epidemiologic study is to determine whether thyroid disease is increased among persons exposed to the releases of radioactive iodine from Hanford between 1944 and 1957. The Study will be completed in late 1998.
References
Freshley MD, Thorne PD. Groundwater Contribution to Dose from Past Hanford Operations. HEDR. August, 1992: PNWD-1974.
Heeb CM. Iodine-131 Releases from the Hanford Site, 1944 through 1947. HEDR. October, 1992: PNWD-2033, Volume I.
Heeb CM. Radionuclide Releases to the Atmosphere from Hanford Operations, 1944-1972. HEDR. May 1994: PNWD-2222.
Heeb CM, Bates DJ. Radionuclide Releases to the Columbia River from Hanford
Operations, 1944-1971. HEDR. May 1994: PNWD-2223.
Napier BA. Determination of Key Radionuclides and Parameters Related to Dose from the Columbia River Pathway. HEDR. March 1993: BN-SA-3768
Napier BA. Determination of Radionuclides and Pathways Contributing to Cumulative
Dose. HEDR. December, 1992: BN-SA-3673.
Napier BA. Selection of Dominant Radionuclides for Phase 1 of the Hanford Environmental Dose Reconstruction Project. HEDR. July, 1991: PNL-7231.
Steele KD. Secrecy Slowing Radiation Study, Researcher Says. Spokane Spokesman-Review. July 16, 1993: B-1.
MODULE 4
Basics of Radiation Epidemiology
by Steve Wing, Ph.D.
Department of Epidemiology, School of Public Health,
University of North Carolina
OBJECTIVES
After studying this module, the reader will be able to
* describe the explanatory approach generally used in radiation epidemiology
* understand and discuss conceptual and technical issues in radiation epidemiology
* identify the practical and theoretical limitations of the approaches utilized in radiation epidemiology
Introduction
Epidemiology is the study of health and disease in populations. Prior to World War II the field was primarily concerned with infectious diseases, and it is from the study of epidemics that the field draws its name. Epidemiological research now addresses a broader range of topics, including environmental agents such as ionizing radiation.
The goals of this module are to describe: (1) the explanatory approach generally used in radiation epidemiology and (2) the practical and theoretical limitations to this approach. The focus on the logic of explanation is intended to encourage critical evaluation of potentials and limitations of epidemiological studies.
The Logic Of Explanation In Radiation Epidemiology
Most investigation in radiation epidemiology addresses questions about the association between radiation exposure, or dose to certain tissues, and an outcome. For example, the relationship between a specific form of ionizing radiation and occurrence of a particular medical outcome is studied. The method of epidemiology is to observe whether disease occurs more or less commonly among individuals who have the exposure or factor than among those who do not. Risk-factor epidemiology explains disease in populations by enumerating all the risk and protective factors, the independent variables or causes, and their relationships with a list of disease outcomes derived from clinical practice, the dependent variables, or effects.
The randomized experiment serves as a model or ideal design for the evaluation of specific agents. First, subjects with specific characteristics, including absence of a disease or outcome of interest, are chosen for study. Next, they are randomized to be exposed or unexposed to a factor, a process that tends to produce an even distribution of the heterogeneous study subjects between exposure groups over the course of many trials. During a period of exposure or non-exposure, all other conditions affecting the subjects can be held constant. Finally, the researcher determines the outcome characteristics in members of each group using a standardized protocol.
The analysis of such a study amounts to a comparison of the frequency of the outcomes of interest between the groups. Differences in frequency that persist over many trials, or that are obtained in a small number of large trials, are attributed to the action of the experimental agent. This method is essentially the same approach that is used in toxicological studies of animals. However, humans should not be experimentally exposed to potentially harmful agents for research purposes. Consequently, most epidemiological studies are observational in nature.
Observational studies attempt to imitate the controlled experiment by making exposed and unexposed groups as similar as possible, except that one group has the exposure itself. This is accomplished both through the design of the study and through statistical analysis of the data. An occupational study of the effects of whole-body exposure to gamma radiation on cancer rates might be designed to include only workers of a certain type; for example, males who worked longer than six months at a specific facility. This avoids some initial differences between exposure groups. The study then might compare workers who had received different cumulative radiation exposures within strata of age, other occupational exposures, and behavioral attributes of interest. This provides a summary estimate of the exposure-disease relationship "adjusted" for differences in those other factors. In attempting to yield results that would have been obtained in an experiment, the observational study attempts to control "extraneous" factors.
It is assumed that well-designed studies can provide an estimate of the radiation-cancer dose-response relationship that characterizes the change in cancer rates for each unit change in radiation. It is often assumed that this is a universal dose response law that could be identified by experimental studies if those were possible [Wing, 1994]. However, many observational studies lack measurements or estimates of individual doses. The disease experience of an entire group of potentially-exposed individuals, such as workers or downwinders, must be compared to some "standard" or "expected" disease rates. Although such studies may identify an excess or deficit of disease, they cannot generally provide information about dose response [Shleien et al., 1991].
Identification of a risk factor or disease agent using the approach based on experimental logic is accomplished by noting a higher disease rate (or excess of observed compared to some predicted number of cases) among an exposed group compared to an unexposed group. However, within the exposed group there is no way to distinguish cases that would not have occurred in the absence of exposure from cases that would have occurred anyway. Thus, risk-factor epidemiology is about factors associated with excess disease in groups. It cannot specify the cause of any particular case of disease.
Some factors associated with disease rates are viewed as causal while others are viewed as spurious. Causal means that the factor acts to create disease. Spurious means that the association occurs either because of another factor or because disease leads to the presence of the factor. This is an overly simplistic view of complex causation of disease within an organism or of disease rates in a population. Nonetheless, this focus on finding exposure-disease associations and then distinguishing causal from non-causal exposures has dominated thinking in modern risk-factor epidemiology.
Limitations In The Epidemiological Approach
Studies of radiation and cancer conducted among Japanese atomic bomb survivors and nuclear workers show that generic difficulties related to comparability, measurement, and knowledge of what to measure pose conceptual and technical problems for radiation epidemiology.
Comparability
Comparability refers to the similarity of individuals with different degrees of exposure. When exposure groups are comparable in other respects, exposure becomes a more plausible explanation of differences in disease rates than when groups differ in other respects. If groups differ in potential to develop cancer, or in exposures to other carcinogens or susceptibility factors, then the absence or presence of a radiation-cancer association of a given form could be due to these other factors.
For many scientists, studies of survivors of the atomic bombing of Hiroshima and Nagasaki have played a dominant role in the assessment of radiation health effects [BEIR V, 1990]. The special circumstances of their exposure in 1945, and survival for inclusion in the population assembled for epidemiological study five years later, may make radiation-disease associations look quite different than they would in other situations. Biased conclusions about the radiation-cancer association in other populations could occur if groups with different degrees of radiation exposure are not comparable in other respects.
Stewart and Kneale [1993a] have presented evidence that differential mortality from the time of the bombing in 1945 until the assembly of the population for epidemiological study in 1950 produced more highly selected groups of robust individuals at higher than at lower exposures. The more robust survivors at higher dose groups would reduce the apparent radiation effect. Further differences among survivors of different levels of exposure may relate to long-term effects of radiation on immune function. This situation raises questions about the applicability of radiation-cancer associations among atomic bomb survivors to other populations. A critical review of the use of atomic bomb survivors as a standard for evaluating radiation health effects is found in Nussbaum and K�hnlein [1994].
Different issues of comparability arise in studies of workers exposed to low-level radiation. To begin with, workers must be healthy enough to be employed. Some studies compare workers with each other rather than with the general population in order to avoid problems of comparability between workers and non-workers. However, workers that enter and remain in jobs involving radiation exposure differ from workers in other jobs; for example, they may have different work skills and preparation. Employers use medical exams to screen workers for dangerous or high-security jobs, and prohibit smoking in some work areas. This could lead to health differences between unexposed workers and those employed in jobs that entail greater radiation exposure.
In one study, workers in jobs with potential for internal contamination with radionuclides had lower mortality from cardiovascular disease and all causes of death combined (but not cancer) than workers who had never been monitored. This suggests general health differences [Wing et al., 1991]. Selective occupational exposure also occurs because occupational exposures accumulate gradually over many years or decades. Only workers healthy enough to remain employed for many years generally reach higher dose levels, while workers who leave employment early due to illness or other reasons generally have lower doses. Workers exposed to radiation may also be exposed to chemical carcinogens, and they may have different smoking or dietary patterns.
Measuring Exposure and Disease
A second major problem in the technical practice of radiation epidemiology is dose measurement. It is important to correctly categorize individuals into groups based on their dose in order to avoid under- or over-estimating an association. Even if disease rates increase with dose, the increase cannot be detected if enough people are incorrectly categorized. This situation leads to "false negative" studies.
Dose estimates for A-bomb survivors were derived from models which consider the amount and energy of radiation released from the bombs and interview data on location and shielding collected five or more years after the bombing. The accuracy of physical models is called into question by several recent changes in estimates of the amount and types of radiation released [BEIR V, 1990; Straume et al., 1992]. Dose misclassification would also result from the use of retrospective survey data used to locate individuals at the time of the bombing.
Workers at some Department of Energy facilities have been issued personal dosimeters to monitor external penetrating radiation exposures, a seemingly ideal measurement situation. However, changes over time in who was monitored, the sensitivity of dosimeters, and the frequency of reading dosimeters can affect the reliability of recorded doses. In the early years, dosimeters were read daily or weekly to help quickly identify workers with higher exposures. But frequent reading may not allow dosimeters to be sufficiently exposed to reach the detection threshold. Doses well below exposure standards have not been of regulatory concern, but are of epidemiological interest, especially when they are accumulated over many years. Other errors occur because of difficulties in matching hundreds of thousands of dosimeter readings collected over many decades to thousands of workers, failure of workers to wear the correct badges, equipment errors, and variation in reading instruments [Wing et al., 1994].
Personal dosimeters do not detect radiation dose from internally-deposited radionuclides. Estimates of doses from internally-deposited radionuclides are made based on information about the solubility of the compounds, the amount excreted in urine and feces, and values for internal transport and residence times derived from models based on clinical studies. Estimates can also be made using whole-body counters that detect the penetrating radiation emitted by the internally-deposited particles. Still, most epidemiological studies of nuclear workers have not quantified internal doses. In any case, the estimates used to classify individuals' doses, as is necessary in an epidemiological study of the exposure-response relationship, are based on a variety of assumptions. This means that quantification of dose-response relationships is speculative and leaves many unanswered questions.
The ability of an epidemiological study to quantify radiation risks also depends on measurement of the outcome. Radiation epidemiology has focused on outcomes such as cancer and major birth defects which are easier to count than some other illnesses. Studies using cancer as an outcome measure usually rely on cancer mortality rather than cancer incidence. Reporting of deaths is legally required and death certificates are gathered in a central registry, but not all states have tumor registries. Death certificates often fail to yield information on cancers that are in remission, unrelated to the primary cause of death, or undetected at the time of death from other causes. The poor quality of death certificate diagnoses remains a problem [Jablon et al., 1990].
What to Measure?
A more fundamental problem in dose-response assessment is the inadequacy of the theoretical basis for knowing what to measure. It is uncertain which aspects of a dose need to be quantified in order for a study to be sensitive to complex radiobiological effects. Among workers exposed to penetrating ionizing radiation over long periods, for example, the total cumulative dose over a worker's employment history is typically studied. Sometimes only the doses received up to a certain number of years in the past are considered in forming exposure groups. These "lag" or "latency" analyses are based on the assumption that cancers take time to develop and that recent exposures are not relevant to disease.
Alternatively, doses received in the distant past might not be etiologically important. The doses that should be counted might be those accumulated around the time of the emergence of the hypothetical mutations leading to radiogenic cancer [Pearce, 1988; Stewart and Kneale, 1993b]. Then again, it might not be the cumulative dose that is critical, but whether the dose is delivered in one or a few short time periods, or is drawn out slowly. Chronic exposures might have a greater opportunity to impact an organism during especially susceptible states, or, in some systems, could allow defense mechanisms to operate. Other aspects of dose that might be important to measure are the peak dose or the coincidence of radiation with other carcinogens or susceptibility states.
Another difficulty in interpreting radiation-cancer associations is that the mechanisms of radiocarcinogenesis are not well understood. Also, there is increasing evidence to suggest that there is variation in the extent to which different cancers are radiogenic. Unlike difficulties of lack of comparability and measurement that may be substantially reduced in experimental settings, the problem of measuring the right thing affects the controlled experiment just as seriously as the observational study.
Epidemiologists know well the problems discussed above of comparability, sometimes called confounding and selection factors, and measurement errors that distort dose-disease relationships. The solutions are to improve measurement, to select study subjects in a way that makes them more comparable, and to statistically adjust for remaining sources of non-comparability that can be identified and quantified. Refinement of epidemiologic method has occurred, and the field has contributed to knowledge about many pathogenic agents, including ionizing radiation. Epidemiological techniques are well-suited to documenting strong risk factors, such as regular cigarette smoking or high-dose ionizing radiation, that show little or minor variation in impact in various population subgroups.
Epidemiological methods, however, are not well-suited for assessing radiation health effects when doses are low and measurements are poor. Relatively small differences in disease occurrence, such as those that are suspected in the case of many environmental radiation exposures, are difficult to detect [McMichael, 1989]. But small increments in disease incidence can have a great population impact when many people are exposed [Rose, 1992]. These are the very situations that are often of most concern to the public and most commonly seen by clinicians.
Other modules in this monograph summarize the research findings of many radiation epidemiology studies. Ironically, studies of downwinders, whose exposures are the focus of the Hanford Health Information Network, are among the most ambiguous of radiation epidemiology studies. The ambiguity derives from all the generic problems reviewed above. Factors contributing to ambiguity include: migration; the long delays between time of exposure and manifestation of a health effect such as cancer; and lack of measurements of the exposures of interest.
Conclusion
Epidemiology's major contribution to the understanding of radiation health effects is the identification of "late effects" of radiation exposure in human populations. Epidemiological studies have observed long-term differences in disease, primarily cancers, associated with radiation exposures. Epidemiological studies are important because of the uncertainties involved in extrapolating health effects from animals to humans, especially when the latency period between exposure and clinical appearance of disease exceeds the life span of most experimental animals.
However, epidemiological studies have important limitations. They generally do not address the reasons for any specific case of disease. Many serious conditions have received little or no attention. Epidemiology's ability to identify an association between exposure and disease is sensitive to the knowledge about which aspects of exposure to measure, the quality and completeness of the exposure and disease measures, and the comparability of the groups being studied. Low-level effects are especially difficult to detect, and there has been relatively little attention to possible subgroups that may be more sensitive to radiation than other groups. Although there has been much excitement about new molecular methods in epidemiology, these new techniques have promised much more than they have delivered [Pearce et al., 1995].
There is often a demand for epidemiological studies when populations have been exposed and there is public concern about such problems. Such studies can be helpful in documenting relationships between specific agents and disease rates when good measurements of both can be made and when sufficiently large numbers of people can be studied. However, when exposures are low and the disease of interest can arise in the absence of exposure, measurement quality must be high and large numbers of people must be studied. In the case of Hanford downwinders, individual doses are especially difficult to document due to uncertainties about what was released; chaotic and complex environmental distribution; and variability in individuals' diets, home, work, physical activity, and biological processing.
Large and expensive historical epidemiological studies may compete for funding with environmental clean-up or clinical services, and such studies may not have the power to detect existing associations. In some cases it has been argued that such studies are funded for the very reason that they are unlikely to detect effects [Sterling, 1980].
As in all areas of science, the construction and interpretation of evidence from epidemiological studies reflects the social context in which the research is produced [Wing, 1994]. Political and economic interests in nuclear industries, including military, energy, and medical uses, have created especially obvious social influences on studies of radiation health effects. However, ionizing radiation exposures are only one of the many important ways that radiation-producing industries affect public health. Health professionals, scientists, policy makers, and activists should consider radiation exposures in the context of these more global issues.
REFERENCES
Committee on the Biological Effects of Ionizing Radiations. Health Effects of Exposure to Low Levels of Ionizing Radiation (BEIR V). Washington, DC: National Academy Press, 1990.
Jablon S, Thompson D, McConney M, Mabuchi K. Accuracy of Cause-of-Death Certification in Hiroshima and Nagasaki, Japan. Ann NY Acad Sci. 1990;609:100-109.
McMichael AJ. Setting Environmental Exposure Standards: The Role of the Epidemiologist. Int J Epidemiol. 1989;18:10-16.
Nussbaum R, K�hnlein W. Current Perspectives on Low-Dose Health Effects of Ionizing Radiation: Consistencies, Discrepancies and Open Questions. Env Health Persp. 1994;102(8):656-667.
Pearce N. Multistage Modeling of Lung Cancer Mortality in Asbestos Textile Workers. Int J Epidemiol. 1989;17:747-752.
Pearce N, Sanjose S, Boffetta P, Kogevinas M, Saracci R, Savitz D. Limitations of Biomarkers of Exposure in Cancer Epidemiology. Epidemiol. 1995;6(2):190-194.
Rose G. The Strategy of Preventive Medicine. NY: Oxford Press, 1992.
Schleien B, Ruttenber AJ, and Sage M. Epidemiologic Studies of Cancer in Populations Near Nuclear Facilities. Health Physics. 1991;61:699-713.
Sterling TD. The Health Effects of Low-Dose Radiation on Atomic Workers: A Case of Employer-Directed Research. International Journal of Health Services. 1980;10:37-46.
Stewart A, Kneale GW. A-bomb Survivors: Further Evidence of Late Effects of Early Deaths. Health Phys 1993a;64:467-472.
Stewart A, Kneale GW. The Hanford Data: Issues of Age at Exposure and Dose Recording. PSR Quarterly. 1993b;3:101-111.
Straume T, Egbert SD, Woolson WA, Finkel RC, Kublik PW, Gove HE, Sharma P, Hoshi M. Neutron Discrepancies in the DS86 Hiroshima Dosimetry System. Health Physics. 1992;63:421-26.
Wing S. Limits of Epidemiology. Medicine and Global Survival. 1994;1:74-86.
Wing S, Shy C, Wood J, Wolf S, Cragle D, Frome E. Mortality among Workers at Oak Ridge National Laboratory: Evidence of Radiation Effects in Follow-up through 1984. JAMA. 1991;265:1397-1402.
Wing S, West CM, Wood JL, Tankersley W. Recording of External Radiation at Oak Ridge National Laboratory: Implications for Epidemiological Studies. J Expos Assess Environ Epidemiol. 1994;4:83-93.
Module 5:Radioactivity in the Body
Module 6:Radiation Dose Estimates from Hanford Radioactive Releases: 1944-1972
Module 8:Genetic Effects and Birth Defects from Radiation Exposure
After studying this module, the reader will be able to
* describe how internal exposure to radionuclides occurs
* explain how the body handles internally-deposited radioactivity
* identify which organs received the main dose from the radionuclides for which the Hanford Environmental Dose Reconstruction Project is estimating doses
Introduction
Production of plutonium at the Hanford Site released over 100 radioactive substances into the environment for more than 40 years. Some substances contributed more than others to the radiation dose a person received. This module discusses how exposure to radiation occurs, how the body handles internal radiation exposure, and which tissues and organs received the main dose from radioactive materials released from Hanford.
How Radiation Exposure Occurs
In addition to Hanford radiation, radiation exposure comes from a variety of sources. These include medical uses of radiation; radioactive substances found in the environment, such as radon or cosmic rays; and nuclear fallout. This module, however, focuses on internal exposure from radionuclides released from Hanford.
Radiation exposure can be either external or internal. External exposure occurs when the radiation source is outside the body. Examples of this kind of exposure include standing in a cloud of radioactive gas, swimming in radioactively contaminated water, or being subjected to X-rays.
Internal exposure occurs when a radionuclide is ingested, inhaled, or enters the body through breaks in the skin. For most people exposed to Hanford's radioactive releases, the main route of exposure was internal for most of the radionuclides listed in Tables 1 and 2 in this section.
The Hanford Environmental Dose Reconstruction Project (HEDR) estimates that six radionuclides released into the air account for nearly all the radiation dose a person may have received through the air pathway. (For a description of the Dose Reconstruction Project, please see Module 3.) Five radionuclides are estimated to account for most of the dose a person may have received from the river pathway. These radionuclides are listed in Tables 1 and 2. Representative dose estimates for the eleven radionuclides are available from HEDR.
HEDR estimates that iodine-131 accounts for most of the radiation dose people received from the air releases. Most of this dose came from eating locally-grown, leafy green vegetables and fruit, as well as drinking milk containing iodine-131. Drinking Columbia River water and eating radioactively-contaminated fish were the two most important factors contributing to radiation dose from Hanford's river releases.
What The Body Does With Radioactivity
Once a radionuclide is inside the body, some of it may enter the bloodstream. The chemical properties of the radionuclide determine how the body handles the radioactivity. The body does not recognize the difference between a radioactive and non-radioactive substance. For example, strontium-90 is chemically similar to calcium and the body utilizes strontium in the bone in much the same way it does calcium.
When a radionuclide concentrates primarily in one organ, as when strontium concentrates in the bone, that organ receives a larger dose from the radioactive substance than do other organs or tissues. Other radionuclides, such as neptunium-239, which are not chemically similar to substances needed for the body's functioning, may also concentrate in different organs or tissues.
Some radioactive substances do not concentrate in one organ, but are distributed throughout the body. Tritium, for example, is a form of hydrogen. Hydrogen is part of the water molecules present throughout the body, so tritium delivers a dose to all tissues.
The dose to different parts of the body is determined by a number of factors, including the amount of radioactivity present and its distribution, solubility in the bloodstream, and the type and energy of the emitted radiation. Once the radioactive substance is taken into the body, it will continue to give off radiation until either the radioactivity has decayed or the body has eliminated the substance through normal metabolism. Both of these processes occur simultaneously.
The rate of decay of a substance depends on its half-life; the amount of time it takes for a radioactive substance to lose one-half of its radioactivity. Half-lives for different substances vary from millionths of a second to billions of years. An atom is no longer radioactive when it decays and becomes stable.
A radionuclide may be absorbed by organs and tissues other than the one in which it concentrates. The radioactive substance will give a radiation dose to the other organs or tissues, but the dose is typically much smaller. Iodine-131, for example, is concentrated by the thyroid gland, but also gives a dose to other organs and tissues, such as reproductive organs and breast tissue. However, the dose from iodine-131 received by the reproductive organs and breast tissue is much less than the dose to the thyroid. For example, the dose to breast tissue is 30,000 times less than the dose to the thyroid. A radiation dose to the ovary is nearly one million times less than a dose to the thyroid.
Hanford's Releases And Radiation Dose
According to 1994 dose estimates from HEDR, releases from Hanford resulted in whole-body doses of 30 rem EDE or less. A whole-body dose is one in which approximately the same dose is received by each organ, as may happen with exposure to tritium. But some people-particularly those living near Hanford before 1960-may have received high doses to the thyroid gland or other organs. Doses to the thyroid gland between 1944 and 1951, for example, may have been as high as 870 rad for some children.
Both whole-body doses and organ doses increase a person's risk of cancer or other health problems. A radiation dose from the radioactive substances released from Hanford may have caused or could cause health problems. Because individuals were exposed to varying amounts of radioactive substances from the Hanford Site over many years, health effects may have resulted. However, very little is known from human health studies about low-dose radiation and health problems other than cancer. Current research methods may not be sensitive enough to detect a link between low-dose radiation and other health problems, if they exist. Hanford-related studies now underway may increase our knowledge about radiation doses and the relationship between iodine-131 doses and thyroid disease. Additional studies may help to identify other health problems reported by some people who were exposed to Hanford's releases.
Tables 1 and 2 refer to radioactive substances released into the air and into the Columbia River. The Tables list the current estimated amount of each substance released from Hanford (1944-1972), the main routes of exposure for each radioactive substance, the organs which received the main dose from the substance, and the physical half-life of each substance. Module 2 introduces the discussion of radiation health effects. Module 7 presents guidelines for evaluation of thyroid disease in people exposed to I-131. Modules 10 and 11 present discussions of possible health effects of exposure to selected radionuclides.
| Substance | Amount Released from Hanford | Main Routes of Exposure | Organs Receiving Main Dose | Half-life |
| Iodine-131 | 739,000 curies | ingestion | thyroid | 8 days |
| Ruthenium-103 | 1,160 curies | external inhalation | whole body lungs | 39.4 days |
| Ruthenium-106 | 388 curies | inhalation/ ingestion | lungs GI tract | 368 days |
| Strontium-90 | 64.3 curies | ingestion | bone surfaces red bone marrow | 28.8 years |
| Plutonium-239 | 1.78 curies | inhalation | lungs bone surfaces | 24,100 years |
| Cerium-144 | 3,770 curies | inhalation
ingestion | lungs
GI tract | 284 days |
| Substance | Amount Released from Hanford | Main Route of Exposure | Organs Receiving Main Dose | Half-life |
| Phosphorus-32 | 229,000 curies | ingestion | red bone marrow | 14.3 days |
| Zinc-65 | 491,000 curies | ingestion | whole body | 245 days |
| Arsenic-76 | 2,520,000 curies | ingestion | GI tract
stomach for infants | 26.3 hours |
| Sodium-24 | 12,600,000 curies | ingestion | stomach | 15 hours |
| Neptunium-239 | 6,310,000 curies | ingestion | GI tract | 2.4 days |
REFERENCES
Heeb CM. Radionuclide Releases to the Atmosphere from Hanford Operations, 1944-1972. HEDR. January, 1994: PNWD-2222.
Heeb CM, Bates DJ. Radionuclide Releases to the Columbia River from Hanford Operations, 1944-1971. HEDR. January, 1994: PNWD-2223.
Phipps AW, Kendall GW, Stather JW, Fell TP. Committed Equivalent Organ Doses and Committed Effective Doses from Intakes of Radionuclides. National Radiological Protection Board of the United Kingdom. 1991: NPRB-R245.
Roessler G. Radiation Dose. (A newsletter by the Technical Steering Panel of the Hanford Environmental Dose Reconstruction Project.) October, 1993.
Till J, Meyers HR, (eds.) Radiological Assessment: A Textbook on Environmental Dose Analysis. U.S. Government Printing Office. Washington, D.C. 1983.
MODULE 6
Radiation Dose Estimates from Hanford Radioactive Releases
by Genevieve Roessler, Ph.D.
Member of the Technical Steering Panel
OBJECTIVES
After studying this module, the reader will be able to
* define the meaning of "source term"
* explain factors contributing to the uncertainty about dose estimates
* understand and discuss the representative dose estimates from the air and river pathways
Introduction
On April 21, 1994, the Technical Steering Panel (TSP) of the Hanford Environmental Dose Reconstruction Project released draft reports. These reports contain dose estimates for representative individuals from radioactive materials released to the air and the Columbia River by Hanford operations from 1944 to 1992.
The highest estimated doses were received by people living downwind of Hanford who drank milk from cows grazing on fresh pasture that was contaminated with iodine-131 from air releases during the time period 1944-1947. Most of the iodine-131 consumed by people concentrated in the thyroid gland. Very young children likely received the highest doses. The TSP also released dose estimates for the radionuclides considered to be the most important in the air and river pathways. The five other air pathway radionuclides are strontium-90, ruthenium-103, ruthenium-106, cerium-144 and plutonium-239. The radionuclides important in the river pathway are sodium-24, phosphorus-32, zinc-65, arsenic-76 and neptunium-239 (Technical Steering Panel, 1994).
This module will discuss the process used to estimate Hanford doses and the unique aspects of this project. The results of both the air pathway and the river pathway dose estimates are summarized. Dose Reconstruction Air Pathway
The first part of the Hanford dose reconstruction was to determine the source term. This process reconstructed how much material was produced in the nuclear reactors and transferred to the chemical separations plants. Scientists then estimated how much radioactive material was discharged to the air. The next part of the reconstruction, called transport and deposition, calculated the concentration of the materials in the air. It also tracked the movement of the materials in time and space and determined the amount deposited on the soil and vegetation.
Scientists next determined the amount of environmental accumulation of the radionuclides in grass, milk, vegetables, and other foods. Dose estimates were then made using lifestyle information, such as food consumption rates, for average or typical groups of people. Much of this work was done using computer models. Lifestyle information for Native Americans was not considered in this part of the study but will be included at a later date.
River Pathway
Source term data for the river pathway provided estimates of the amount of radioactive material discharged to the Columbia River. Project scientists used source term estimates for the eight Hanford nuclear reactors operating from January 1950 through January 1971 to estimate the concentrations of key radioactive materials in the Columbia River water. Scientists estimated the concentrations for several downstream locations by simulating radioactive material flow and transport in the river. A computer program simulated transport of the five specific river pathway radionuclides from the Hanford reactors to the mouth of the Columbia River. A simplified model was used to estimate doses for the years 1944-1949. Dose estimates for 1971 to 1992 used data from Hanford annual environmental reports.
Monthly average water concentrations were reconstructed for 12 sections of the Columbia River for the five radionuclides contributing the most to dose. Actual monitoring data were used when available. Where actual monitoring data were limited, radionuclide water concentrations were estimated by using estimates of releases from the reactors along with information about dilution in the river. These water concentrations were used, along with water pathway lifestyle information, to calculate dose estimates for representative individuals. Unique Aspects Of The Hanford Environmental Dose Reconstruction Project
The information needed to calculate the true dose any one person received does not exist. Actual monitoring data are limited, and the amount of environmental radioactive contamination at any given place and time can only be estimated, not determined. Radiation doses also depend on factors unique to each person, some of which cannot be recalled exactly. As a result, there will be some uncertainty about the true dose that each person actually received. In addition, since the dose estimates are generated by computer models, it is important to validate the models' abilities to predict results.
Uncertainty/Sensitivity Analysis
Uncertainty in dose estimates can be caused by several factors. These include incomplete information, such as not being able to measure all the food people actually ate, and errors made in past measurements of radioactive materials in emissions, the environment, or people. Natural variations also contribute to uncertainty in the input information used in the computer models for doing dose calculations. Examples of these variations include differences among individuals in age, sex, lifestyle, and geographic location; differences among dairy cows in the amounts of contaminated pasture grass they ate; and differences in milk production of individual cows during the year.
Project scientists assessed these factors to determine the level of uncertainty for each. For the release of iodine-131 to the air, for all cases, the factor contributing the most to uncertainty-30 to 70 percent-is the difference in the way a person's body takes up ingested radioactive material. This results from differences such as variations in the size of the thyroid and metabolism. For representative individuals drinking milk from family cows fed fresh pasture, the second most important factor is the difference in the way radioactivity is transferred from the feed to a cow's milk. This contributes 35 to 40 percent of the overall uncertainty. Validation
Scientists validate the accuracy of the computer model used to estimate doses by comparing the computer-estimated concentrations with actual measurements obtained from the field or laboratory. These include measurements of radioactive materials in the environment (vegetation, fish, and Columbia River water) and in Hanford workers and school children; and limited, past dose estimates for the public.
Compilation of a sufficient number of these validations was done to demonstrate the general reliability of the project's dose estimation methods. As a result of the model validation work to date, no revisions to any of the models were recommended by the TSP.
Doses From The Hanford Air And River Pathways Air Pathway
Scientists calculated air pathway dose estimates for people exposed to the radioactive releases during the years 1944 to 1992. The dose estimates are for representative (or typical) individuals who lived in a 75,000 square mile area surrounding Hanford.
Exposures of the thyroid to iodine-131 dominated the doses in the air pathway. Detailed iodine-131 dose estimates were prepared for the years 1944 through 1951 covering 1102 locations. Doses to twelve different kinds of representative individuals, distinguished by age and gender, were estimated for a series of food source scenarios. These dose estimates were presented in a report as a series of maps showing annual or cumulative absorbed dose to the thyroid (Farris, et al. 1994). Figure 1 is a map of the cumulative median thyroid doses of a representative child with the maximum exposure from all air exposure pathways for the years 1944 through 1951 when the iodine-131 releases were the highest.
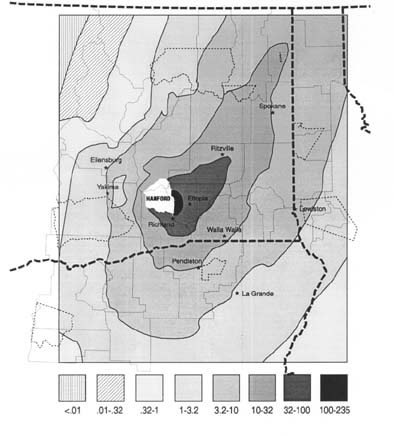
To use the map, locate the area of interest, note the shading, and in the key find the dose range that corresponds to the shading. For each shaded area, there is a range of median doses in the key. The maximally-exposed representative individual is estimated to have been a child at Ringold, Washington, born in 1944 and remaining at that location through 1951. The median dose for this maximally-exposed child is 240 rad, with a dose range of 54 rad to 870 rad.
The cumulative thyroid doses calculated for downwind areas near Hanford were larger than those more distant from the site. Table 1 shows doses for a maximally-exposed child in other locations.
Doses also vary with age and sex due to different diets and different metabolism of materials in the body. In general, doses are somewhat higher in males than females and go down as age progresses for individuals with the same location and diet pattern. The source of a person's milk has a large impact on doses.
Persons drinking milk from cows that grazed on fresh pasture generally have the highest doses, whereas those drinking milk from cows that ate stored feed have lower doses. Commercial milk yielded lower doses than backyard cows as a result of partial decay of iodine-131 during processing and distribution or when milk produced in different locations was combined. Generally, people who drank commercial milk have an estimated dose lower than the dose to persons who drank milk from cows fed solely on fresh pasture and higher than the dose to persons drinking milk from cows fed solely on stored feed.
When milk is not a part of a person's diet, the major contributor to dose is the consumption of fresh leafy vegetables. The doses from fresh leafy vegetables are much smaller than those from milk.
The annual and cumulative doses for a representative adult from 1945-1972 for five other important radionuclides were calculated. However, iodine-131 was the dominant radioactive material contributing to dose during all of the 1940s and 1950s. In 1945, iodine-131 exposure was responsible for 99.8 percent of the dose to an adult in Richland, Washington, if that person drank fresh milk from a cow on pasture. Plutonium-239 and cerium-144 were the next largest contributors at about 0.1 percent of the total dose each.
| Location | Median Dose | Dose Range |
| Ringold | 235 rad | 54 rad to 870 rad |
| Richland | 93 rad | 24 rad to 350 rad |
| Eltopia | 73 rad | 19 rad to 300 rad |
| Ritzville | 28 rad | 7.4 rad to 120 rad |
| Walla Walla | 13 rad | 3.7 rad to 44 rad |
| Spokane | 11 rad | 2.8 rad to 44 rad |
| Pendleton | 8.6 rad | 2 rad to 30 rad |
| Lewiston | 4 rad | 1 rad to 15 rad |
| Yakima | 2.8 rad. | 66 rad to 9.6 rad |
| Ellensburg | 2.1 rad. | 52 rad to 6.7 rad |
By 1965, iodine-131 releases had decreased to the point where cerium-144 became the dominant contributor to dose and was dominant for the remainder of the time period examined. Nevertheless, over the entire period of 1945 to 1972, iodine-131 was by far the dominant radioactive material contributing to dose at 98.8 percent.
These dose estimates may change somewhat as the work of the dose reconstruction project continues. Additional study of plutonium and ruthenium particles released from the stacks of two Hanford plants is planned.
Possible Health Effects from the Air Pathway
Estimating one's dose from historical Hanford operations is one area of interest. Many people ask what these doses mean to their health. One method of putting radiation doses to the thyroid in perspective is to compare doses from Hanford's releases to medical diagnostic procedures. In the past, doctors used iodine-131 in nuclear medicine tests to see whether the thyroid was functioning properly. In this procedure, the thyroid typically received a radiation dose of 50 to 100 rad.
A retrospective cohort study by Holm et al [1988] investigated the incidence of thyroid cancer in people examined with diagnostic doses of iodine-131. The researchers concluded there was little evidence that iodine-131 is carcinogenic in humans at diagnostic doses. In a critique of this study, Gofman [1990] disagrees. His analysis of study data indicated an excess of thyroid cancer. One of the reasons for the differing analyses is that the Holm study excluded thyroid diseases diagnosed during the first five years after initial administration of iodine-131. This was done to account for the possibility of cancer being present but undiagnosed at the time of testing and not detected clinically until some years later. Gofman's analysis of the data includes thyroid diseases diagnosed within the first five years after administration of iodine-131.
Studies of low-dose exposures are necessary to further knowledge about the effects of iodine-131. Results of the Hanford Thyroid Disease Study may provide specific information about the risk of thyroid disease among people exposed to Hanford's radioactive releases.
The doses from the other air pathway radionuclides were typically in the low millirem EDE to fractions of a millirem EDE range (for an explanation of EDE, please see "Radiation Dose Units"). It is difficult to say much about the health effects of these radionuclides as there are few studies of internal exposure at low-dose levels. However, most scientists agree that any radiation exposure has a potential for causing health effects, such as cancer. River Pathway
The highest radiation doses received by people from the Columbia River pathway were generally much smaller than the highest doses from the air pathway. There are many reasons for this. Two are most important. First, many radioactive elements which were released to the river have short half-lives. Since it often takes longer for materials to reach people by water than by air, more of the radioactivity will have decayed by the time people come in contact with the radioactivity. Second, concentrations of radioactive material in drinking water or fish were likely much lower than concentrations in cow's milk or leafy vegetables.
Detailed dose estimates for the time period of the largest releases, 1950-1971, were calculated on a monthly basis for three types of individuals for 12 sections of the Columbia River. The doses were highest during this time period because the radioactive releases were at their peak.
Doses were calculated for a "maximum representative individual," a "typical representative individual," and an "occupational representative individual."
The "maximum" individual ate three meals of resident fish per week, drank treated Columbia River water, and spent some recreational time on or near the river. The "occupational" individual spent an average of more than 55 hours per week on or in the river and drank only untreated river water. This individual ingested some salmon and shellfish but no resident fish. The "typical" individual, based on historical surveys, did not eat resident fish or consume large quantities of untreated river water.
Table 2 shows median doses for each of these representative individuals for 12 sections of the river. Doses are shown for three periods (1944-49, 1950-71, and 1972-92) and cumulatively for 1944-92. These EDE doses summarize doses from all radiation sources in an equivalent way.
| Location | 1944-49 | 1950-71 | 1972-92 | Total (1944-92) | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| M | T | O | M | T | O | M | T | O | M | T | O | |
| Ringold | 103 | 8 | 32 | 1421 | 51 | 519 | 7 | 4 | 7 | 1531 | 63 | 558 |
| Richland | 100 | 7 | 27 | 1393 | 29 | 908 | 7 | 4 | 7 | 1500 | 40 | 942 |
| Kennewick/Pasco | 91 | 6 | 22 | 1297 | 63 | 507 | 7 | 4 | 7 | 1395 | 73 | 536 |
| Snake/Walla Walla | 60 | 4 | 14 | 881 | 44 | 290 | 4 | 3 | 4 | 945 | 51 | 308 |
| Umatilla/Boardman | 59 | 3 | 10 | 709 | 26 | 101 | 4 | 3 | 4 | 772 | 32 | 115 |
| Arlington | 53 | 3 | 8 | 683 | 24 | 87 | 4 | 3 | 4 | 740 | 30 | 99 |
| John Day/Biggs | 52 | 3 | 7 | 667 | 23 | 79 | 4 | 3 | 4 | 723 | 29 | 90 |
| Deschutes River | 49 | 3 | 7 | 629 | 22 | 73 | 4 | 2 | 4 | 682 | 27 | 84 |
| The Dalles/Celilo | 48 | 2 | 6 | 618 | 21 | 70 | 4 | 2 | 4 | 670 | 25 | 80 |
| Klickitat River | 46 | 2 | 5 | 597 | 20 | 64 | 4 | 2 | 4 | 647 | 24 | 73 |
| Cascade Locks | 44 | 2 | 4 | 575 | 19 | 58 | 4 | 2 | 4 | 623 | 23 | 66 |
| Lower River | 36 | 1 | 3 | 456 | 15 | 41 | 3 | 2 | 3 | 495 | 18 | 47 |
Radiation Dose Units
Scientists measure radiation in dose units. These dose units help assess and describe the potential damage to body tissues by radiation.
One key unit is a rad. This unit of dose describes how much energy body tissues absorb during an exposure. The radiation dose it describes is called "absorbed dose."
However, equal absorbed doses of different types of radiation may not produce equal effects on the body. An absorbed dose of alpha particles is more damaging than the same absorbed dose of gamma rays or beta particles. To account for this difference, a unit of dose called "dose equivalent" is used. Its unit of measurement is the rem.
To determine the dose equivalent, absorbed dose must first be calculated. Absorbed dose is then multiplied by a radiation weighting factor depending on the type of radiation. The radiation weighting factor for alpha particles is 20. To calculate the dose equivalent for an exposure to alpha particles, the dose in rad is multiplied by 20 to give the dose equivalent in rem. For gamma rays and/or beta particles, the radiation weighting factor is one. In this case, 1 rad is equal to 1 rem.
Another factor is important in evaluating radiation exposure. Different parts of the body respond differently to the same dose of radiation as some body cells are more sensitive to radiation than others. In some cells, radiation is more likely to cause late effects, such as cancer, or genetic changes.
The same radiation dose has different impacts on different parts of the body. To account for these variations, individual tissues are given weighting factors which take into consideration the level of impact of a given radiation dose on a tissue of interest. Parameters that were taken into account in developing the weighting factors include the probability that radiation will induce a particular type of cancer or genetic effect, the probability that the cancer or effect will be lethal, and the years of life that will be lost as a result of the death. These tissue weighting factors are as follows:
Gonads 0.25
Red bone marrow 0.12
Lung 0.12
Breast 0.15
Thyroid 0.03
Bone surface 0.03
Colon, stomach, bladder, 0.05
liver, esophagus, skin (each)
It can be implied, for example, that the gonads, with a weighting factor of 0.25, are more than twice as likely to suffer a health impact from the same dose than the red bone marrow or the lung.
If all of these weighting factors are added up for the 12 tissues, the total comes to 1.00. This allows a uniform comparison of the impact of the irradiation of an individual tissue to that of the irradiation of the whole body.
Another special dose is called effective dose equivalent (EDE). It is used when weighting factors are taken into consideration. The name-effective dose equivalent-is appropriate since it states that it is not only the dose that is taken into consideration but also the effect or the impact on the tissue of interest. The unit of effective dose equivalent is also the rem and is often called the rem EDE.
To use this approach, one must calculate the absorbed dose (rad) and then convert it to dose equivalent (rem). Assume that the absorbed dose calculated to the thyroid for an individual exposed to iodine-131 is 100 mrad. The dose equivalent is 100 mrad multiplied by the radiation weighting factor for iodine-131, a beta emitter, which is one. This is then multiplied by the tissue weighting factor for the thyroid of 0.03 to give the effective dose equivalent.
100 mrad x 1 = 100 mrem Dose Equivalent
100 mrem x 0.03 = 3 mrem Effective Dose Equivalent (EDE)
This can be interpreted by saying that the expected health impact on an individual of an absorbed dose to the thyroid of 100 mrad is about 1/30th of what it would be if the whole body received an absorbed dose of 100 mrad.
If a number of organs or tissues are irradiated, their contribution to the effective dose can be added up to produce the total effective dose equivalent. For example, assume the thyroid receives 100 mrem, the lungs receive 200 mrem, and the gonads receive 10 mrem:
Thyroid 100 mrem x 0.03 = 3.0 mrem
Lungs 200 mrem x 0.12 = 24 mrem
Gonads 10 mrem x 0.25 = 2.5 mrem
Total Effective Dose Equivalent = 29.5 mrem
REFERENCES
Davis E, Kopecky KJ, Hamilton TE, Amundson B. Hanford Thyroid Disease Study: Study Protocol. Centers for Disease Control. Atlanta, Georgia. 1993.
Farris WT, Napier BA, Ikenberry TA, Simpson JC,. Shipler DB. Atmospheric Pathway Dosimetry Report, 1944-1992. HEDR, Battelle, Pacific Northwest Laboratory, Richland, Washington. 1994: PNWD-2228.
Farris WT, Napier BA, Ikenberry TA, Simpson JC, Shipler DB. Columbia River Pathway Dosimetry Report, 1944-1992 HEDR, Battelle, Pacific Northwest Laboratory, Richland, Washington. 1994: PNWD-2227.
Gofman J. Radiation-Induced Cancer from Low-Dose Exposure: An Independent Analysis. San Francisco: Committee for Nuclear Responsibility. 1990.
Holm LE, et al. Thyroid Cancer after Diagnostic Doses of Iodine-131: A Retrospective Cohort Study, Journal of the National Cancer Institute. 1988; 80(14): 1132-1138.
Technical Steering Panel. Representative Hanford Radiation Dose Estimates. Washington Department of Ecology, Nuclear Waste Program, P.O. Box 4761, Olympia, WA 98504-7651. 1994.
MODULE 7 Recommended Guidelines for Evaluation of Thyroid Disease in Person Potentially Exposed to Environmental Radioiodine
by the Hanford Thyroid Disease Study OBJECTIVES
After studying this module, the reader will be able to
* discuss guidelines from the Hanford Thyroid Disease Study for the evaluation of thyroid disease in people exposed to environmental iodine-131
* name the initial diagnostic procedure for evaluation of a thyroid nodule
Background
Atmospheric Releases of Radioactive Iodine from the Hanford Nuclear Reservation
In February 1986, the Department of Energy released 19,000 pages of documents, some previously classified, that detailed the environmental records of past emissions at Hanford. Among the most serious problems disclosed in these documents were the airborne releases of iodine-131. The most current information from the Hanford Environmental Dose Reconstruction (HEDR) Project estimates that approximately 737,000 curies of iodine-131 were released from the Hanford Nuclear Site in the 1940s and 1950s.
This information, as well as the current information from two large ongoing scientific studies investigating these emissions, has led to widespread public concern about effects of these releases on the health of people who have lived in the region around Hanford. In particular, questions have arisen from both the public and the medical community as to the types of thyroid problems which may have resulted from these exposures, as well as which type of screening evaluations is recommended.
The purposes of these physician guidelines are to give the medical community some background about radiation-induced thyroid disease, provide recommendations for clinical evaluation of thyroid disease, and to summarize the two major ongoing scientific studies.
Radiation-Induced Thyroid Disease
The primary evidence linking exposure to ionizing radiation with the subsequent development of thyroid disease results from studies of individuals exposed to head and neck radiation in childhood, as well as from studies of Japanese atomic bomb survivors. The treatments during childhood were formerly given to children for benign diseases of the head and neck. Examples of the indications for head and neck radiation treatments included: presumed enlargement of the thymus gland, tonsillar enlargement, acne, cervical adenitis (such as with individuals having tuberculosis), and fungal infections of the scalp.
The type of radiation utilized for such treatments during childhood was external gamma radiation. These external beam treatments were generally directed toward the head and neck and were often given on multiple occasions.
Since the 1950s, it has become apparent that such treatments increased the risk of developing both benign and malignant thyroid tumors. There is also evidence which shows that such exposures increase the risk of hypothyroidism.
The radioactive material released from the Hanford Nuclear Site that is of greatest concern in the context of thyroid disease is iodine-131. The radiation exposure described in the preceding paragraphs is from external gamma rays or X-rays. Most of the radiation dose for iodine-131, however, is due to beta radiation from iodine-131, which is concentrated in the thyroid gland.
Much less information is available in the scientific literature to suggest that iodine-131 exposure produces thyroid tumors in human beings. The available information is primarily from patients with hyperthyroidism who are treated with iodine-131. This information shows that at high doses of iodine-131 the thyroid gland can be ablated, resulting in hypothyroidism. There is little information to indicate that such iodine-131 treatments increase the risk of developing thyroid tumors. However, this has been clearly shown in animal studies. It has also been suggested from recent studies of persons exposed to atmospheric nuclear testing at the Nevada Test Site that iodine-131 may cause an increased risk of developing thyroid neoplasms.
While there has been a dramatic increase in childhood thyroid cancer in persons exposed to fallout from the Chernobyl accident, it is not yet certain which type of radiation or combination of radiation types have caused these cancers.
As a result of the above information, it can be stated with confidence that thyroid tumors, both benign and malignant, and hypothyroidism can result from exposure to external radiation. Regarding radioactive iodine exposure, while it is certain that hypothyroidism can result from sufficient doses of iodine-131, the question of benign or malignant thyroid tumor development after iodine-131 exposure remains uncertain.
Approach to the Evaluation Of Thyroid Disease and Recommendations to Persons Potentially Exposed to Environmental Radioiodine
We recommend the following approach for individuals having any concerns that they may have a thyroid problem or concern that they may have been exposed to radioactive iodine releases from Hanford. The first recommendation is that they see their personal or family physician or other health care provider for an evaluation. This applies not only to persons who may have symptoms or may feel ill, but also to individuals who are asymptomatic, but who are concerned that they may have a thyroid problem.
Second, some individuals may feel that if their health care provider is not an expert in radiation issues, they will not be able to evaluate thyroid problems that might have resulted from Hanford emissions. It is our belief and recommendation to both the public and the medical community that the evaluation of thyroid disease is the same regardless of whether the thyroid problem might have been caused by radiation exposure or might be totally unrelated to such exposure. Therefore, it is not necessary to consider a health care provider's expertise in health physics or radiation issues when deciding whom to see for a thyroid evaluation.
Third, we recommend to the medical community that consultants in endocrinology or internal medicine be liberally utilized, either for interpretation of abnormal screening results or for more experienced thyroid examinations.
Clinical Evaluation Of Thyroid Disease
The following is the recommended minimum evaluation for an individual concerned about the possibility of a thyroid problem.
Incorporated into these recommendations is a complete history and physical examination, given that many symptoms and signs of thyroid dysfunction overlap with other medical problems.
A.Complete history with elaboration of residence history; prior endocrine, thyroid, or parathyroid problems; prior history of childhood head and neck radiation treatments; prior thyroid diagnostic tests; and a prior history of thyroid or neck surgery.
B.Complete physical examination, including careful thyroid examination.
C.Laboratory to include free thyroxine index (total thyroxine level and T3 resin uptake) and TSH level.
D.Thyroid nuclear scans or thyroid ultrasound scans are NOT recommended as routine initial screening diagnostic tests. However, they may be utilized as an additional evaluation once a thyroid problem is clinically suspected.
E.Although there is some variation in the diagnostic evaluation of a thyroid nodule, the initial diagnostic procedure is fine needle aspiration biopsy of the thyroid nodule.
F.In individuals who have a normal screening evaluation for thyroid disease, it is recommended that they be rescreened on a yearly basis, or less often as indicated by the health care provider. This would be particularly true in those individuals who have reason to believe that they may have been exposed to environmental radioactive iodine.
G.Follow-up of abnormal screening evaluation: as noted, above, liberal use of consultants in endocrinology or internal medicine is recommended. Studies
A.Hanford Environmental Dose Reconstruction (HEDR) Project. This study was begun in 1987 and the technical work was conducted by Battelle Pacific Northwest Laboratories under the direction of an independent Technical Steering Panel (TSP). This dosimetry study seeks to estimate the radiation dose that persons living around Hanford may have received from the release of radioactive emissions into the air, ground water, and the Columbia River. The primary efforts of this study have focused on the estimation of radiation doses to the thyroid that people may have received from exposure to radioactive iodine. Battelle reported the results of its work in April 1994. The Technical Steering Panel evaluated these results and completed additional technical tasks during 1994 and 1995.
B.Hanford Thyroid Disease Study (HTDS). This study, authorized by an act of Congress in 1988, was funded by the Centers for Disease Control and Prevention and is being conducted by the Fred Hutchinson Cancer Research Center in Seattle, Washington. The primary purpose of this epidemiologic study is to determine whether thyroid disease is increased among persons exposed to the releases of radioactive iodine from Hanford between 1944 and 1957. The Phase II feasibility study began in December 1992 and was completed in December 1994. A full epidemiologic study was completed in 1998.
Bruce Amundson, M.D.
Robert Griep, M.D.
Thomas Hamilton, M.D., Ph.D.
Hanford Thyroid Disease Study
Fred Hutchinson Cancer Research Center
Seattle, Washington 98104
MODULE 8 Genetic Effects and Birth Defects from Radiation Exposure
OBJECTIVES
After studying this module, the reader will be able to
* name three birth defects that may result from in utero exposure to radiation
* identify the genetic effect associated with paternal pre-conception radiation exposure
* discuss the association between radiation and genetic effects indicated by studies of children born to atomic bomb survivors
* describe to patients, in general terms, genetic effects and birth defects from radiation exposure
Introduction
People exposed to Hanford's radioactive releases have many questions and concerns about radiation's effects on their personal and family health. A key concern is whether radiation from Hanford caused genetic effects or birth defects.
This module discusses genes, mutations and birth defects, and how radiation can harm a cell. Summaries of studies of the effects of pre-conception parental radiation exposure, the effects of in utero radiation exposure, and results from new laboratory research are included. The findings of these studies are considered in relation to Hanford's releases.
Introduction To The Basics Of Genetic Effects And Birth Defects
The deoxyribonucleic acid (DNA) in each cell of an individual consists of segments called genes. Genes are part of the 23 pairs of chromosomes found in human cells. Mutations in the genes can arise spontaneously or as a result of exposure to radiation or chemical and physical agents. When these changes result from radiation exposure they are called radiation-induced mutations.
A germline mutation, or inheritable genetic effect, occurs when the DNA of a reproductive cell is damaged. A somatic mutation, which is not inheritable, occurs when the DNA of a non-reproductive cell is damaged.
Radiation-induced germline mutations may cause health problems which include miscarriages, stillbirths, congenital defects, neonatal or infant death, chromosomal abnormalities and cancer in later life. Radiation-induced somatic mutations affect only the exposed individual and may also cause health problems (see Module 2).
Birth defects can arise spontaneously, through radiation-related impairment of normal developmental processes, or can be induced by other toxic exposures. A birth defect caused by a germline mutation from parental pre-conception exposure is an inherited genetic effect. In utero fetal exposure can result in errors in development that may manifest themselves as retardation in physical growth or mental development.
Birth defects that may result from in utero fetal exposure to radiation include a reduction in standing and sitting height, severe mental retardation, microcephaly and impairment of brain development, which may indirectly reduce an individual's intelligence quotient (IQ) and school performance.
How Radiation Can Harm A Cell
When a radioactive particle or wave hits a cell in the body, one of four things may occur:
* it may pass through the cell without doing damage;
* it may damage the cell, but the cell may be able to repair the damage before it produces new cells;
* it may kill the cell; or
* it may damage the cell in such a way that the damage is passed on when new cells are formed.
Studies Of Genetic Effects And Birth Defects From Exposure To Radiation
Most research of radiation and genetic effects and birth defects involves exposure to external radiation, such as X-rays. In contrast to this external exposure, nearly all of the dose from Hanford came from internal exposure. That is, people were exposed to this radiation through the food and water they consumed and the air they breathed.
The results of studies of external exposure may not apply to people exposed to internal radiation. Also, an internal exposure from a radioactive substance may give a dose mainly to one organ, such as iodine-131 gives to the thyroid. Internal radiation exposure may have different genetic effects than those of external radiation exposure.
Pre-conception Parental Radiation Exposure Children of Hanford Workers
Studies by Sever and others [1988] reported an association between neural tube defects and the radiation dose fathers received before their children were conceived. This effect was observed in children whose fathers received low doses (10 rem or less) of external whole-body radiation while working at Hanford. These results were not supported by studies of children born to atomic bomb survivors who received higher doses of radiation.
Other research suggests that pre-conception parental radiation exposure can increase the frequency of birth defects; further studies are underway. One study being conducted around the Hanford Site is investigating the relationship between parental exposure to radiation and leukemia in their children.
Children Born in the Hanford Area
Sever and others [1988] also conducted a study of birth defects in Washington's Benton and Franklin counties near Hanford. The researchers examined the number of cases of certain birth defects between 1968 and 1980. There were more neural tube defects than expected when the county rates were compared with rates from Washington, Oregon, and Idaho. Cleft lip was reported less often in Benton and Franklin counties than in the three-state area.
Using information from a study of Hanford workers, the researchers concluded that the increase in neural tube defects was not explained by parental employment at Hanford or by occupational exposure to radiation. The researchers also concluded it was unlikely that exposure of the general public to radiation from Hanford operations caused the increase in neural tube defects. This conclusion was based on a dose estimate of slightly more than 1 rem for the years 1974-1980.
This Hanford study includes only a few years relevant to the Hanford Health Information Network, with its Congressional mandate to focus on 1944-1972, the years of the largest releases. In addition, the dose estimate for the public includes only the years 1974-1980, during which there were limited Hanford operations. Also, the study was conducted prior to any dose estimates being available from the Hanford Environmental Dose Reconstruction Project (HEDR). (For a description of HEDR, please see Module 1.)
Japanese Atomic Bomb Survivor Studies
Otake [1989, 1993], Yoshimoto [1988, 1990], Schull [1984], and others have reported on genetic studies of children whose parents were exposed to the Hiroshima and Nagasaki atomic bombs. There was essentially no difference between the rate of inherited birth defects in children whose parents were exposed to radiation and in controls whose parents were not exposed. These researchers, however, believe that genetic damage did occur because of the radiation exposure. Animal research and laboratory experiments suggest that inherited genetic effects from radiation exposure should occur in humans. It is possible that current research methods may not be able to detect the genetic effect in humans.
Cancer Survivors
Mulvihill and Byrne [1987] conducted a follow-up study of cancer survivors who had undergone radiotherapy or chemotherapy. They investigated whether the offspring of the cancer survivors had higher rates of genetic disease than children of parents without cancer. People in the study group were diagnosed with cancer before the age of 20 and had survived for more than five years. The researchers compared the study group to a control group. The rates of genetic diseases were the same in both the group of cancer survivors and the control group indicating that there was not a higher rate of genetic disease in children of cancer survivors who had undergone radiotherapy or chemotherapy or both.
Effects Of In Utero Radiation Exposure
Research suggests there is a relationship between in utero X-ray exposure and development of childhood cancer. A large study by Stewart [1956] and another by MacMahon [1962] found an association between medical X-ray exposure before birth and childhood cancer. These findings indicate that the most sensitive period of exposure for developing leukemia is the first half of the third trimester of pregnancy. The first and second trimesters of pregnancy are the most sensitive for developing all cancers except leukemia.
Studies of children born to mothers who received whole-body radiation doses of between 50 and 100 rad following the Japanese atomic bombing showed that the children experienced an increased risk for microcephaly and mental retardation. This was especially true for those women who were 8 to 15 weeks pregnant at the time of exposure. Compared with non-exposed children, these children exposed to whole-body radiation doses during this period in utero had lower intelligence test scores and performed less well in school. Atomic bomb survivor studies also suggest that children exposed to radiation in utero have cancer rates equal to or higher than children who were exposed from ages one to nine.
Leukemia In Children Born To Radiation-Exposed Fathers
In 1990, Gardner and colleagues published the results of a study of leukemia and non-Hodgkin's lymphoma among young people born and living near the Sellafield nuclear power plant in West Cumbria, United Kingdom. The researchers concluded that leukemia in children was linked to their fathers' exposure to external whole-body radiation before conception of the child.
For children whose fathers worked at the nuclear facility, the rate of childhood leukemia was twice as high as normal. There was also an eightfold increase of leukemia in children whose fathers received a lifetime dose greater than 10 rem or a dose greater than 1 rem within the six months before the children's conception. Leukemia, however, was also found more often than expected in children whose fathers were farmers or worked in the steel or chemical industries.
Interpretation of this finding includes consideration of the very small number of fathers whose children had leukemia. Only 4 out of 46 fathers who worked at Sellafield and had a radiation dose greater than 10 rem were compared to 3 out of 276 control group fathers.
Several scientists attempted to reproduce the results of Gardner's study. A study by McKinney [1991] indicated a 2.5-fold increase in leukemia in children whose fathers had radiation doses similar to those in the Gardner study. But Urquhart [1991] found that there was a 42 percent reduction in leukemia in children of exposed fathers compared with unexposed fathers.
Other scientists have developed different explanations about the results of Gardner's study. Evans [1990] found that most of the children had a genetic disorder that caused acute lymphatic leukemia and that this disorder was not related to a father's radiation exposure. Kinlen [1990] suggested that the increase in leukemia was due to a virus and found increased childhood leukemia in children born in other towns.
A number of scientists have concluded that Gardner's finding is not biologically plausible. Although the researchers Doll and Darby [1994] believe that Gardner's finding is biologically possible, they disagree with Gardner's conclusion. They argue that the conclusion is not supported by what is currently known about radiation genetics, or the inherited nature of childhood leukemias or studies of the children of atomic bomb survivors or nuclear facility workers. Doll and Darby conclude that the association between a father's radiation exposure and leukemia is a chance finding.
Sorohan and Roberts [1993] evaluated the relationship between childhood leukemia and a father's pre-conception radiation exposure. Using data already collected for the Oxford Survey of Childhood Cancer, researchers estimated a father's radiation dose based on his reported occupation. The researchers found little support for a father's exposure to external whole-body radiation in the six months before a child's conception as a risk factor for childhood cancer. The study suggested, however, that a father's internal exposure to radionuclides was connected with childhood cancer risk more often than exposure to external whole-body radiation.
Laboratory Experiments And Genetic Effects
Laboratory experiments suggest that plutonium-238 may produce genetic damage in cells. Kadhim [1992] reported that alpha particles from plutonium-238 produced a high frequency of chromosome damage in descendants of cells grown in the laboratory. Research by Hatsumi and Little [1992] indicates that alpha particles from plutonium-238 can cause genetic damage in the chromosomes of a cell for doses as small as 0.03 rem (30 mrem).
These findings from laboratory studies suggest that plutonium-238 can possibly induce genetic effects in humans from small doses of radiation. Two factors need to be considered when interpreting these findings: (1) genetic damage is constantly being repaired by the cells themselves, and (2) laboratory experiments with cells cannot be used to predict exactly what might occur in cells inside the human body.
Tawn and colleagues [1985] studied the chromosomes of white blood cells in plutonium workers. Chromosomal aberrations, or changes, were found. This suggests a relationship between plutonium exposure and genetic effects.
Scientists do not agree on the significance of some chromosomal aberrations. One perspective is found in a report issued by a National Academy of Sciences committee [1990] that studied the biological effects of ionizing radiation. The scientists commented that the implications, if any, of an increase in chromosomal aberrations in white cells are not clear. Another perspective is offered by Gofman [1992]. He argues that if aberrations increase in white cells, they also increase in other cells including reproductive cells. In Gofman's opinion, many birth defects considered to be of unknown origin result from chromosomal damage induced by radiation.
Animal studies, mainly using mice, have detected genetic effects not detected in human studies. This may suggest that humans are less sensitive to radiation than mice. Since genetic mutations are found in all animal species studied, it is expected that mutations do occur in humans.
Summary of Studies
Animal research and laboratory experiments suggest that radiation-induced inherited genetic effects should occur in humans. However, studies of the offspring of the Japanese atomic bomb survivors do not detect inherited genetic effects. Some studies suggest that a paternal pre-conception exposure to radiation may cause leukemia in the child, while others suggest this effect does not occur. Exposure to radiation in utero is linked to problems such as childhood leukemia, mental retardation, small head size, and lower IQ.
Genetic Effects, Birth Defects and Hanford
In comparison to the doses of most groups studied for genetic effects and birth defects, the Hanford dose estimates are generally considered low. This does not rule out the possibility that genetic effects and birth defects might be caused by exposure to radiation from Hanford. Some people exposed to Hanford's releases may have received doses equal to or higher than doses in the large study by Stewart. This study associated in utero X-ray exposure with leukemia in children. However, the effects of exposure to X-rays may not predict the effects of exposure to the substances released from Hanford.
In April 1994, HEDR released a draft of dose estimates for representative individuals. According to these estimates, even people who received the highest exposures were in the low-dose category for whole-body exposure (below 50 rem).
HEDR developed dose estimates for six radioactive substances released into the air: iodine-131, plutonium-239, ruthenium-103, ruthenium-106, strontium-90, and cerium-144. Iodine-131, which concentrates in the thyroid gland, accounts for most of the dose to most people from the air pathway. The highest estimated dose to the thyroid was for a child between 1944 and 1951 and was 870 rad. This is equivalent to an estimated whole-body dose of 29 rem EDE (Effective Dose Equivalent). A typical person who was an adult by 1944 had a cumulative estimated whole-body dose from exposure to all six air pathway substances of 1 rem EDE from 1944 to 1972.
For releases into the Columbia River, HEDR made dose estimates for five radioactive substances: zinc-65, phosphorus-32, neptunium-239, sodium-24 and arsenic-76. The highest estimated cumulative dose to an adult's red bone marrow was 2.8 rem EDE, and 4.8 rem EDE to the lower large intestine. The highest estimated cumulative whole-body dose for an adult was 1.4 rem EDE.
Conclusion
As with other health effects from radiation, it is assumed that any exposure to radiation carries some risk of genetic effects and birth defects. There are many questions regarding the association between radiation exposure and genetic effects and birth defects. Additional studies are necessary before the magnitude of the risk can be determined.
NOTES
The HEDR Project was formed in 1987 to estimate radiation doses the public may have received as a result of releases of radioactive materials from the Hanford Site. The Project was initially funded by the U.S. Department of Energy (DOE) and later funded by the U.S. Centers for Disease Control and Prevention (CDC).
REFERENCES
Bross IDJ, Natarajan N. Genetic Damage from Diagnostic Radiation. JAMA. 1977; 237:2399.
Bross IDJ, Natarajan N. Genetic Damage in Children Exposed to Preconception, and Intra-uterine Radiation. Investigative Radiology. 1980; 15(1):52.
Byrne J, Mulvihill JJ, Myers MH, Connelly RR, et al. Effects of Treatment on Fertility in Long-term Survivors of Childhood or Adolescent Cancer. N Engl J Med. 1987; 317:1315-1321.
Carr DH, Gedeon M. Population Cytogenetics of Human Abortuses, pp. 1-9. In: Population Cytogenetics: Studies in Humans. (EB Hook and IH Porter, Eds). New York: Academic Press. 1977.
Committee on the Biological Effects of Ionizing Radiations. Health Effects of Exposure to Low Levels of Ionizing Radiation (BEIR V). Washington, DC: National Academy Press, 1990.
Doll R, Evans HJ, Darby SC. Paternal Exposure Not to Blame. Nature 1994; 367 (February 24): 678-680.
Evans HJ. Leukemia and Radiation. Nature. 1990; 345:16-17.
Gardner MJ, Snee MP, Hall AJ, et al. Results of Case-control Study of Leukemia and Lymphoma among Young People Near Sellafield Nuclear Plant, West Cumbria. British Medical Journal. 1990; 300:423-429.
Gofman JW. No One Escapes Harm: The Essential Story of In-Utero Irradiation. Committee for Nuclear Responsibility. November 1992.
Gofman JW. Radiation-Inducible Chromosome Injuries: Some Recent Evidence on Health Consequences-Major Consequences. Committee for Nuclear Responsibility. Spring 1992.
Hatsumi N, Little JB. Induction of Sister Chromatid Exchanges by Extremely Low Doses of A-Particles. Cancer Research. 1992; 52:6394-6396.
Kadhim MA, MacDonald DA, Goodhead DT, et al. Transmission of Chromosomal Instability after Plutonium A-Particle Irradiation. Nature. 1992; 355:738-740.
Kinlen LJ, Clarke K, Hudson C. Evidence from Population Mixing in British New Towns 1946-85 of an Infective Basis for Childhood Leukemia. Lancet. 1990; 336:577-582.
Kneale GW, Stewart AM. Childhood Cancers in the UK and Their Relation to Background Radiation. In: Radiation and Health: The Biological Effects of Low-Level Exposure to Radiation. (RR Jones and R Southwood, Eds). Chichester (UK): Wiley. 1987; Chapter 16:203-220.
Kondo S. Health Effects of Low-level Bomb Effects: Taratogenic Effects. In: Health Effects of Low-level Radiation. Madison: Medical Physics Publishing. 1993. Macht SH, Lawrence P. National Survey of Congenital Malformations Resulting from Exposure to Roentgen Radiation. Am J Roentgenology 1955: 73 (3).
MacMahon B. Prenatal X-ray Exposure and Childhood Cancer. J Natl Cancer Institute. 1962:1173-1191.
McKinney PA, Alexander FE, Cartwright, et al. Parental Occupations of Children with Leukemia, West Cumbria. British Medical Journal. 1991; 303: 681-687.
Mulvihill JJ. Sentinel and Other Mutational Effects in Offspring of Cancer Survivors. In: Mutation and the Environment. (Eds, ML. Mendelsohn and RJ Albertini). Part C. New York, Wiley. 1990.
Neel JV. Commentary, "Update on the Genetic Effects of Ionizing Radiation," JAMA. August 7, 1991.
Otake M, Schull WJ. Radiation-related Small Head Sizes among Prenatally Exposed A-Bomb Survivors. Int'l J Radi Biol.1993; 63:255-270.
Otake M, Schull WJ, Neel J. Congenital Malformations, Stillbirths, and Early Mortality among Children of the Atomic Bomb Survivors: A Reanalysis. Radiation Effects Research Foundation (RERF) Technical Report 1989:13-89. [RERF TR 13-89]. Hiroshima: RERF.
Otake M, Schull WJ, Yoshimaru H. A Review of Radiation-related Brain Damage in the Prenatally Exposed Atomic Bomb Survivors. Radiation Effects Research Foundation (RERF) Commentary and Review 1989; Series 4-89. [RERF CR 4-89]. Hiroshima: RERF.
Sankaranarayanan K. Ionizing Radiation and Genetic Risks. IV. Current Methods, Estimates of Risk of Mendelian Disease, Human Data and Lessons from Biochemical and Molecular Studies of Mutations. Mutation Research. 1994; 258:99-122.
Schull WJ. Critical Assessment of Genetic Effects of Ionizing Radiation on Pre- and Post-Natal Development. Issues and Review in Teratology. 1984; 2:325-398.
Sever LE, Gilbert ES, Hessol NA, McIntyre JM. Case-control Study of Congenital Malformations and Occupational Exposure to Low-level Ionizing Radiation. Am J Epidemiol. 1988; 127:226-242.
Sever LE, Hessol NA, Gilbert ES, McIntyre JM. The Prevalence at Birth of Congenital Malformations in Communities Near the Hanford Site. Am J Epidemiol. 1988.
Sever LE. Parental Radiation Exposure and Children's Health: Are There Effects on the Second Generation? Occupational Medicine. 1991; 6:613-637.
Sorohan T, Roberts PJ. Childhood Cancer and Paternal Exposure to Ionizing Radiation: Preliminary Findings from the Oxford Survey of Childhood Cancers. Am J Ind Med. 1993; 23:343-354.
Stewart A, Webb J. Giles D, et al. Malignant Disease in Childhood and Diagnostic Irradiation In Utero. Lancet. 1956; 2:447.
Tawn EJ, et al. Chromosomal Studies in Plutonium Workers. International Journal of Radiation Biology and Related Studies in Physics, Chemistry and Medicine. 1985: May; 47(5):599-610.
TSP, Technical Steering Panel of the Hanford Environmental Dose Reconstruction Project. Summary: Radiation Dose Estimates from Hanford Radioactive Material Releases to the Air and the Columbia River. Richland (WA): TSP. (April 24) 1994.
Urquhart JD, Black RJ, Muirhead MJ, et al. Case-control Study of Leukemia and Non-Hodgkin's Lymphoma in Caithness Near the Dounreay Nuclear Installation. British Medical Journal. 1991; 302:687-691, 818.
Wakeford R, Tawn EJ, McElvenny DM, Binks K, Scott LE, Parker L. The Seascale Childhood Leukemia Cases-The Mutation Rate Implied by Paternal Preconceptional Radiation Doses. Journal of Radiation Protection (UK). 1994; 14:17-24.
Xias OS, et al. A Population Based Case-Control Study of Childhood Leukemia in Shanghai. Cancer. 1988; 62:635-644.
Yoshimoto Y, Kato H, Schull WJ. Risk of Cancer among In Utero Children Exposed to A-Bomb Radiation, 1950-84. Radiation Effects Research Foundation (RERF) Technical Report 1988:4-88. [RERF TR 4-88]. Hiroshima: RERF.
Yoshimoto Y, Neel J, Schull WJ, Kato H, Soda M, Eto R, Mabuchi K. Frequency of Malignant Tumors during the First Two Decades of Life in the Offspring (F1) of Atomic Bomb Survivors. Radiation Effects Research Foundation (RERF) Technical Report 1990;4-90. [RERF TR 4-90]. Hiroshima: RERF.
Module 9:The Nervous System and Radiation
Module 11:Radionuclides in the Columbia River: Possible Health Effects in Humans and Effects on Fish
Module 12:Talking With Patients About Radiation Health Effects: Case Histories and Discussion
OBJECTIVES
Glossary After studying this module, the reader will be able to
* identify the health effects to the nervous system connected with high-dose and low-dose radiation exposure
* describe the results of a study concerning birth defects of the nervous system in children of Hanford workers
Introduction
Some people believe there is a higher-than-usual rate of nervous system disorders among individuals exposed to Hanford's releases of radioactive materials. This module summarizes research about disorders of the nervous system. Researchers know more about how high-dose radiation affects the nervous system than about how low-dose radiation affects it. Researchers also know more about exposures from external sources than from radioactive substances acting within the body. Hanford's releases, however, resulted in low whole-body doses from mainly internal exposure, according to estimates of the Hanford Environmental Dose Reconstruction Project (HEDR). Nonetheless, to understand the range of potential health effects, it is useful to look at what is known about the health effects of high-dose radiation from external exposures.
Health Effects Of High-Dose Radiation
High doses of radiation can be defined as greater than 50 rem to the whole body. High-dose radiation is used to treat cancer. In the past it was used to treat benign conditions such as ringworm of the scalp and enlargement of the thymus gland in the neck. Some Japanese atomic bomb survivors, nuclear industry workers, and survivors of nuclear accidents also received high doses of radiation.
Health effects in people exposed to high radiation doses include effects on the brain, spinal cord, and peripheral nerves.
Effects on the Brain
People treated with radiation for brain tumors often receive doses of a few thousand rad to the head, usually over a period of days or weeks. Health effects that can occur within days or weeks of treatment include swelling of the brain, seizures, paralysis, and confusion. Long-term effects that may occur include the destruction of brain cells, changes in the blood vessels of the brain, seizures, and confusion.
Ron et al conducted a study of Israeli children treated with radiation for ringworm of the scalp. The researchers estimated the dose to the brain for this group as between 100 and 200 rad. This group had a higher rate of cancerous and benign brain tumors than unexposed groups.
Other studies have also linked radiation exposure to the development of brain tumors. These were studies of people treated with radiation for conditions of the head and neck, arthritis of the spine, and acute lymphocytic leukemia.
However, studies of Japanese atomic bomb survivors have not reported a link between high-dose radiation exposure and brain tumors.While these studies found no evidence of a radiation effect for brain tumors, there is evidence of an increased risk for other nervous system tumors in people exposed to the atomic bomb explosions before they were 20 years old.
These atomic bomb studies have, however, found measurable nervous system effects on some children born to Japanese women who were pregnant during the bombings of Hiroshima and Nagasaki. The women received whole-body radiation doses ranging from 50 to 100 rad between eight and 25 weeks after conception. The children had an increased risk for small brain size and mental retardation, lower intelligence test scores, and decreased school achievement.
Effects on the Spinal Cord
The spinal cord is generally more sensitive to the acute (short-term) effects of radiation than is the brain. It also takes less time for radiation-induced damage to the spinal cord to show up than similar injury to the brain.
Myelitis, or inflammation of the spinal cord, can occur within two to four months after a patient being treated with radiation is exposed to thousands of rad. Myelitis may have symptoms of tingling, prickling, and shock-like sensations.
Myelitis is sometimes delayed, not occurring until four months to three years after radiation exposure. This delayed effect is due to scarring of the spinal cord and is not a direct effect on spinal cord nerve cells. When delayed, a person may experience more severe problems such as paralysis and lack of bladder control.
Another delayed effect of high-dose radiation exposure to the spine is the development of spinal cord tumors years after the radiation exposure. Effects on the Peripheral Nerves
Peripheral nerves (which connect the brain and spinal cord to other parts of the body) are among the parts of the body most resistant to radiation.Nonetheless, the Israeli children discussed above in the study by Ron and her colleagues had a higher rate of cancerous and benign tumors of peripheral nerves than people not exposed to radiation.
Localized treatment with high doses of radiation has also been reported to injure a group of nerves that extends from the lower neck to the underarm area. This group of nerves is called the brachial plexus.
Health Effects Of Low-Dose Radiation Birth Defects of the Nervous System in Children of Hanford Workers
Lowell Sever and others conducted a case-control study of children born in the Hanford area. The researchers investigated if there was a link between a parent's work exposure to low-level external radiation and birth defects in that worker's children. The study investigated births between 1957 and 1980 since only a few hospital records were available for earlier years.
The researchers found that the higher the radiation dose received by parents before their children were born, the more likely the children were to be born with neural tube defects. Defects of the neural tube--which develops into the spinal cord and brain--occur when the tube fails to close completely during the early stages of pregnancy.
Researchers also reported a link between parental employment at Hanford and two non-neurologic birth defects: congenital dislocation of the hip and tracheoesophageal fistula, an abnormal connection between the trachea (the windpipe) and the esophagus (the part of the digestive tract that connects the mouth to the stomach). However, these two birth defects were not linked with parental exposure to radiation as not all Hanford workers were exposed to radiation at work. Many worked in offices and did not receive any occupational radiation exposure. This study did not include parents' exposure to radioactive materials outside of work, including environmental releases from Hanford, medical procedures, or background radiation.
Birth Defects of the Nervous System in Communities near Hanford
Sever et al also conducted a study of the rate of birth defects in communities near the Hanford Site.The researchers investigated whether rates of birth defects among infants in the Hanford area were higher than expected, potentially because of exposure to radioactivity from Hanford operations.
The researchers determined the rates of certain birth defects for Benton and Franklin counties in Washington state between 1968 and 1980. The Hanford Site covers part of both Benton and Franklin counties. These rates were compared to rates from the Centers for Disease Control's Birth Defects Monitoring Program for Washington, Oregon, and Idaho. While the overall rate of birth defects in Benton and Franklin counties was not greater than expected, the rate of certain neural tube defects was increased.
The researchers compared the study group to other radiation exposed groups. They considered the Hanford doses too low to account for the elevated rates of neural tube defects as being caused by radiation exposure. The researchers did not have an explanation for the elevated rates but proposed that exposure to agricultural chemicals be considered.
The study was conducted before any dose estimates were available from HEDR. Also, the study's dose estimate for the public includes only the years 1974 through 1980, during which there were limited Hanford operations and emissions.
Brain Tumors Among U.S. Nuclear Workers
Deaths from brain tumors are unusual in the general population (4.1 deaths per 100,000 people). In a work force of several thousand, even a small number of cases (two to five) points to a higher number of such deaths than would ordinarily be expected.
Alexander reviewed studies of workers at 10 nuclear facilities. Radiation doses were available for workers at eight of the facilities. For three of the groups, doses included both external and internal exposure. Cumulative average whole-body doses ranged from 0.67 rem to 4.75 rem. There is a small group of workers who had higher doses, perhaps as high as 100 rem. However, individual doses for the workers who developed brain cancer were not provided.
The researcher concluded that there was a higher-than-expected number of deaths from brain cancer among the nuclear industry workers studied. While chemical exposure may contribute to the risk of cancer, the only common factor among the workers was exposure to radiation.
In summary, some researchers have linked certain nervous system health effects to radiation exposure. Health effects linked to high-dose exposure include cancerous and benign brain tumors in people exposed, and small brain size and mental retardation in children of women who were exposed during pregnancy. Health effects linked to low-dose exposure include brain cancer among nuclear industry workers.
Hanford's Releases and the Nervous System
Unfortunately, most of what is known about radiation's effects on the nervous system cannot be directly compared with the Hanford situation. Current knowledge comes from studies of people exposed to high organ doses or high whole-body doses of radiation received over minutes, hours, or days. In contrast, Hanford's releases resulted in some high radiation doses to the thyroid, some low doses to other organs, and low whole-body doses. These doses occurred over weeks, months, or years.
While most studies of radiation's effect on the nervous system involve external exposure, most of the dose from Hanford's releases came from internal radiation exposure. People were internally exposed when they drank contaminated milk or water, or ate contaminated foods. Because the circumstances of the studies discussed above differ from the Hanford situation, the conclusions of those studies do not necessarily apply to Hanford-exposed people.
Occurrence of Nervous System Diseases
Some people believe there is a higher-than-usual occurrence of nervous system diseases among people exposed to Hanford's releases of radioactive materials. Determining the occurrence of nervous system diseases can be difficult. For most of these diseases, only estimates are available of the number of cases in the United States, since there are no requirements to report nervous system diseases to health officials. Little or no information has been collected about the number of cases of many of these diseases among people exposed to Hanford's releases of radioactive materials. As a result, it is not possible, with the information currently available, to determine if the occurrence of nervous system diseases among Hanford downwinders is higher than usual.
Notes
1. Fred A. Mettler and Robert Moseley, Jr. Medical Effects of Ionizing Radiation. San Diego: Grune and Stratton, 1985.
2. Elaine Ron et al. "Tumors of the Brain and Nervous System After Radiotherapy in Childhood." The New England Journal of Medicine; Vol. 319, No. 16, 1988, pp. 1033-1039. Ron is a radiation epidemiologist at the National Cancer Institute in Bethesda, Md.
3. National Research Council. Health Effects of Exposure to Low Levels of Ionizing Radiation (commonly known as BEIR V-the report of the fifth Committee on the Biological Effects of Ionizing Radiations). Washington, DC: National Academy Press, 1990.
4. Shoji Tokuoka and Masayoshi Tokunaga. "Site-Specific Cancer Incidence: An Interim Report." RERF Update; Spring 1995, pp. 6-7. Tokuoka and Tokunaga are with the Department of Epidemiologic Pathology, Radiation Effects Research Foundation (RERF), Japan.
5. Desmond Thompson et al. "Cancer Incidence in Atomic Bomb Survivors, Part II: Solid Tumors, 1958-1987." Radiation Research, Vol. 137, 1994, pp. S17-S67.
6. BEIR V.
7. Mettler and Moseley.
8. Ron et al.
9. Mettler and Moseley.
10. Ron et al.
11. Lowell E. Sever et al. "A Case-Control Study of Congenital Malformations and Occupational Exposure to Low-Level Ionizing Radiation." American Journal of Epidemiology; Vol. 127, No. 2, 1988, pp. 226-242. At the time of this study, Sever was with the Division of Birth Defects and Developmental Disabilities, Center for Environmental Health, Centers for Disease Control in Atlanta, Ga.
12. Lowell E. Sever et al. "The Prevalence at Birth of Congenital Malformations in Communities near the Hanford Site." American Journal of Epidemiology; Vol. 127, No. 2, 1988, pp. 243-254.
13. Victor Alexander. "Brain Tumor Risk Among United States Nuclear Workers." Occupational Medicine: State of the Art Reviews. Philadelphia: Hanley and Belfus, Inc., Vol. 6, No. 4, October-December, 1991, pp. 695-714. Alexander is a researcher with EnviroMedicine Associates in New Orleans, La.
References
HHIN Publications
Genetic Effects and Birth Defects from Radiation Exposure, Fall 1994
The Immune System and Radiation, Summer 1994
Radioactivity in the Body, Spring 1994
From HHIN Articles Available
"Low-Level Ionizing Radiation: Paternal Exposure & Children's Health." Sever, Lowell E. Health & Environment Digest (Freshwater Foundation), February 1991.
Radionuclides in the Columbia River: Possible Health Effects in Humans and Effects on Fish
OBJECTIVES
After studying this module, the reader will be able to
* describe the process that resulted in radioactive contamination of the Columbia River
* provide details concerning how people may have been exposed to radiation
* identify the five radionuclides released into the river pathway and summarize the health effects of exposure to these radionuclides
Introduction
For more than forty years, the U.S. government produced plutonium for nuclear weapons at the Hanford Site in south central Washington state. During that time, Hanford released radioactive elements and other materials into the Columbia River. From World War II until the early 1970s, the Columbia River downstream from Hanford "held the distinction of being the most radioactive river in the United States." Many people now wonder what the potential health effects might be from exposure to these materials. There is also concern about the effects of these releases on the fish population and whether eating contaminated fish increased the risk of adverse health effects in humans.
Hanford discharged three kinds of pollutants into the Columbia River: heat, chemicals, and radioactive material. River water was used to cool the reactors. Before running the water through the reactors, Hanford added chemicals to keep pipes clean in the cooling system. As the cooling water was piped through the reactors, it picked up radiation as well as heat. All three types of pollution were discharged into the Columbia with the cooling water. Because the Network's Congressional mandate directs us to focus on radiation released from Hanford, this report will focus on the radioactive material.
According to the Hanford Environmental Dose Reconstruction Project (HEDR), there were five radionuclides that contributed the most to radiation dose from the river pathway (dose is the amount of radiation absorbed by a person's body). The five radionuclides were phosphorus-32, zinc-65, arsenic-76, neptunium-239 and sodium-24. HEDR estimates that these radionuclides accounted for more than 94 percent of the potential radiation dose from the river pathway. There were many other radioactive materials released into the river as well, but they contributed much less to dose, according to HEDR.
This report examines the releases of these five radionuclides to the Columbia River and the potential health effects which might result from people being exposed to these materials.
What are the possible health problems from exposure to radioactive forms of phosphorus, zinc, arsenic, neptunium and sodium? Most of the information on health effects from these materials has come from research on animals. None of these studies contains information that relates to the specific situation of people who used or spent time on the Columbia downriver from Hanford. While comparisons of these studies to the Hanford situation are uncertain, this report discusses potential health problems which may have been caused or could be caused by exposure to these radionuclides.
How Hanford Radiation Polluted the Columbia
Causes of Contamination
The primary cause of the radioactive pollution of the Columbia River was from the routine operation of the first eight plutonium production reactors. The first three were built during World War II and five more were added between 1949 and 1955. The first reactor began operating in September 1944 and the last one shut down in January 1971.
The nuclear reactions inside these reactors created plutonium and great amounts of heat. The cooling system used water from the Columbia River, ran it through pipes in the core of the reactors, and then back into the Columbia. This process was called "once-through cooling."
There were various chemicals in the cooling water. Some of these occurred naturally in the river water. Others were added to treat the water before it entered the reactors and to keep the pipes of the cooling system clean. Some of these chemicals became radioactive when they were exposed to the intense radiation field in the reactor cores. Some of these chemicals contained phosphorus. Inside the reactor core, some of this phosphorus became radioactive phosphorus-32. As much as 25 to 40 percent of the phosphorus-32 released to the river came from the chemicals used for water treatment. . The rest of the phosphorus that became radioactive was naturally occurring.
After leaving the cores, the discharged cooling water, or effluent, went into retention basins. The purpose of the basins was to allow time for some of the short-lived radiation to decay and the reactor-heated water to cool. The cooling water was near 200oF when it left the reactors. It cooled somewhat while in the retention basins, but was still much hotter than the river temperature when it was discharged back to the river. The basins were designed to have a retention time that ranged from two to six hours. After flowing through the retention basins, the cooling water was discharged into the Columbia River.
In addition to adding five reactors, Hanford increased the power levels of all eight reactors to produce more plutonium for the country's nuclear arsenal. As a result, more radioactivity was discharged into the Columbia. The reactors needed more cooling water to operate at higher levels. The greater flow of cooling water reduced the retention time to as short as twenty minutes. This shorter retention time contributed to more radioactivity entering the river. The radioactive contamination levels in the Columbia River were highest from 1957 to 1964.
The ninth and last plutonium production reactor to be built at Hanford, the N reactor, had a different cooling system than Hanford's first eight reactors. Like commercial nuclear power reactors, N reactor had two cooling systems. The two cooling systems are designed so that the cooling water that is exposed inside the reactor core is not released back into its source. The N reactor, therefore, did not significantly contribute to the pollution described in this report. The N reactor operated from 1963 to 1987.
In addition to the increased power levels and the resulting decreased retention time, there were two other causes of radioactive pollution entering the Columbia River from Hanford. These were fuel element failures and reactor purges.
The nuclear fuel consisted of fuel "elements" which were less than two feet long and encased in metal. There were thousands of fuel elements in each reactor. The increase in the reactor power levels put more stress on the fuel elements. Under this stress, the metal covering could split and allow small chunks of the radioactive fuel to be flushed into the river with the cooling water. The largest chunk weighed more than a pound. There were nearly 2,000 fuel element failures during the operation of the eight original plutonium production reactors.
Purging the reactor piping also contributed to the contamination of the river. Impurities in the cooling water entering the reactor caused a film to build up on the inside of the cooling pipes within the reactor. This film was radioactive. As it built up in the pipes, it increased the radiation exposure to workers in the reactor buildings. Periodically, the piping system was flushed with chemicals to strip off the film. These were called "reactor purges." When the accumulated film was purged, it went through the retention basins, then into the river, and contributed to the contamination of the Columbia.
Factors Influencing Radiation Exposure
In addition to the causes of radioactive contamination discussed above, there were two factors which influenced the amount of radiation people were exposed to: seasonal changes in the Columbia and the addition of dams.
When seasons change, so does the Columbia. In the spring, the river is swollen with runoff from the melting snowpack. There is more water flowing and it is moving faster. This helped dilute the concentration of radioactive material in the river water. The temperature of the water is also affected: cooler in the large flows of winter and spring, warmer in smaller flows of summer and fall. The cooler water of winter and spring decreased the amount of radionuclides absorbed by fish because their metabolisms slowed and they ate less. Summer and fall brought smaller flows, warmer water and a resulting higher concentration of radioactivity. Summer and fall, then, were the times when exposures likely peaked in river areas near Hanford, especially during September, October, and November.
Dams also affected the flow of the Columbia River. In 1944, Bonneville was the only dam downstream from Hanford; by 1971, there were four. The dams changed the way radioactive materials were carried and distributed down the river in two main ways. First, the dams slowed the flow of the river. This slower flow allowed more of the radioactive materials to decay before reaching people farther downstream from the Tri-Cities (Richland, Pasco, and Kennewick). Second, the radioactive materials downstream were further decreased because some adhered to the sediment trapped behind the dams.
In short, Hanford polluted the Columbia River by releasing radioactive materials from the plutonium production reactors. Next, this report will examine how people were exposed to Hanford's radiation from the Columbia River pathway.
How People Were Exposed To Radiation From Hanford
People were exposed to Hanford's radiation via the river pathway if they
* drank contaminated water;
* ate contaminated food (fish, shellfish or waterfowl); or
* spent time along the shoreline of or swam in the contaminated stretches of the Columbia River.
Contaminated drinking water was the largest contributor to a typical person's dose from the river pathway. Eating contaminated foods was the next significant contributor to dose, followed by exposure while boating or swimming. The contribution from eating crops that had been irrigated by Columbia River water was estimated by HEDR to have been so small that it was not included in the dose estimates. People who drank water from the Columbia River downstream of Hanford between 1944 and 1972 would have been exposed to radiation. Some communities drew drinking water from the Columbia. The water treatment system of Pasco had special filters that captured some of the radioactive materials. The city of Richland did not draw its water from the Columbia until October 1963. Prior to this, its water supply came from the Yakima River. Not all cities took drinking water from the Columbia. For example, Portland, Oregon, got its drinking water from a reservoir near Mt. Hood.
Other people drank untreated river water. One example is those who worked on barges transporting goods along the river. The common practice of the barge crews was to drop a bucket into the river to get their drinking water. In 1956, Hanford officials considered issuing restrictions on drinking untreated river water. They concluded that restrictions were "not essential." They also noted that "public relations might suffer from such restrictions."
The second source of exposure in the river pathway was from eating contaminated food: fish, shellfish, and waterfowl. As is discussed later in the next section, Columbia River fish were contaminated.
The radiation in the Columbia also reached the Pacific Ocean, contaminating shellfish along the Washington and Oregon coasts. The levels of zinc-65 in the oysters of Willapa Bay on the Washington coast were monitored beginning in 1959. According to a 1959 Hanford document, the levels of zinc-65 in Pacific oysters were more than 300 times higher than in Japanese or Atlantic coast oysters.
Ducks and geese that nested or fed along the Columbia became contaminated. Waterfowl also picked up radioactivity from waste ponds on the Hanford site. The contamination levels were higher in birds collected on the Hanford site than in those from the areas surrounding Hanford. In early 1970, several ducks collected from waste ponds near the reactors were found to be very contaminated. If someone had immediately eaten one-half pound of the most contaminated duck, the radiation dose to the bone would have been four times higher than the annual acceptable standard at the time.
People with unique lifestyles may have eaten other kinds of contaminated food. For example, Native Americans ate shoreline roots and berries.
The third source of exposure was from spending time along the shore, swimming, or boating downstream from the Hanford reactors. Most of this exposure was in the form of external, whole-body radiation. Some people have recalled that in the 1950s and 1960s, they preferred swimming near Hanford because the water felt warmer there than further downstream.
Hanford and Columbia River Fish
Hanford scientists began studies on Columbia River fish in 1945. They wanted to learn if the reactor effluent, which was discharged to the river, had any effect on fish. They constructed a laboratory at Hanford near the reactors. Young fish were exposed in tanks to various concentrations of effluent, usually at levels much higher than Hanford was releasing to the Columbia River.
There are two kinds of fish in the Columbia River: anadromous and resident. Anadromous fish are those that hatch in fresh water and return there to spawn, but spend most of their lives in the ocean. Some examples of anadromous fish are salmon and steelhead trout. These two types of anadromous fish are the most valuable to the region's economy and to Native Americans.
The early Hanford studies were concerned primarily with young Chinook salmon and steelhead trout. Eggs and young fish were exposed to higher concentrations of effluent than were actually present in the river. Many died. However, Hanford scientists determined that the cause of death was not exposure to the radioactivity. The fish deaths were determined to be due mainly to the chemicals added to pretreat the cooling water and the increase in water temperature. The studies did not examine the long-term effects of exposure in the fish.
When mature anadromous fish return from the ocean to fresh water, they do not feed. Since they are not exposed by eating contaminated smaller fish, they are not thought to accumulate much radioactive contamination. Due to significant public concern, HEDR is planning additional work on the radiation levels that were present in anadromous fish as they came up the Columbia to spawn.
Resident fish are those that live their entire lives in fresh water. Examples of resident fish are crappie, bass, river trout, whitefish, and sturgeon. Due to spending more time in the contaminated portions of the Columbia River than anadromous fish, the resident fish collected higher concentrations of radioactivity. Most of the radiation in the fish came from eating smaller aquatic creatures such as algae and insects. The algae could concentrate the radiation up to 100,000 times the levels of contamination in the river water.
Resident fish in the Hanford area readily accumulated the radioactive phosphorus in their bodies because the levels of natural phosphate in the river were low.The whitefish had the highest concentrations of phosphorus-32. Because of this, Hanford researchers selected whitefish as the focus of their fish monitoring efforts.
The Hanford Health Information Network has received several questions about the radioactivity levels in sturgeon. The concern is raised because sturgeon feed off the bottom of the river where radioactive sediments are found and because sturgeon can live more than 100 years. Based upon studies conducted by Hanford, scientists concluded that eating sturgeon would have given a lower dose than eating crappie, perch, or bass. This lower exposure was due to lower concentrations of radioactivity in the sturgeon and people catching fewer sturgeon than other fish.However, a scenario of a person eating large quantities of sturgeon is entirely reasonable and this diet could have resulted in a higher exposure.
Official Concerns In The Past
Did Hanford pose a danger to the fish and to people who ate fish? The historical record is not consistent. Based on the laboratory studies and the monitoring of the river, Hanford scientists and government officials concluded that "the effluents were diluted to relatively safe levels" based on standards at the time. However, some health officials in the past expressed serious concern about the contamination levels in the Columbia River.
During Hanford's early years, Herbert M. Parker was in charge of the health and safety programs.In 1954, as he considered the projected increases in radiation being released into the Columbia from the reactors, Parker suggested that it might be necessary to impose a public fishing ban from just above Hanford (Priest Rapids) down-river to McNary Dam.Parker noted that the "public relations impact would be severe." According to a report by the Hanford Education Action League, a nonprofit organization based in Spokane, Washington."
Although no fishing ban was ever imposed, the radiation levels in Columbia River fish surpassed the point at which Parker had considered a fishing ban during the years 1957, 1958, 1960, 1961, 1963, and 1964."
Nor was concern focused only on the section of the Columbia nearest to Hanford. In 1964, the U.S. Public Health Service recommended that immediate action be taken to cut in half the radioactivity levels in "the Lower Columbia River." Although not specified in this report, the Lower Columbia was usually referred to as downriver from McNary Dam to below Portland.
urrent Concerns
Many people have expressed concerns about the radioactive materials from past releases that are trapped behind Columbia River dams, especially McNary. However, a Washington Department of Health report has concluded that the risk for adverse health effects is less than that associated with federal and state drinking water standards. This could change if the sediments were dredged (although this is unlikely).
Hanford Dose Estimates
HEDR has calculated "representative dose estimates." For the river pathway, these are estimates of dose for three typical lifestyles with variations in food and water consumption and place of residence.
The lifestyles of actual individuals, such as those who subsisted on fish, might be different than the "representative" categories. Many Native Americans rely heavily on fish, especially salmon, for food. The Columbia River Inter-Tribal Fish Commission (CRITFC) recently surveyed the fish consumption of Native Americans in the Columbia River Basin. The results show that the average fish consumption rate for Native Americans using the Columbia River is "approximately nine times greater" than for the general U.S. population.
Although the Network's previous report on the radionuclides released to the air contained the range of representative dose estimates for each radionuclide, the same level of information for radionuclides released to the river is not available. HEDR's estimates of exposures from the river pathway are generally much lower than those from the air pathway. Because of this, HEDR did not go into as much detail for the dose estimates via the river pathway.
The cumulative (1944-1971) representative dose estimates for adults from the five radionuclides released to the river range from near zero to about 1.5 rem EDE (Effective Dose Equivalent-whole-body dose). The dose estimates to specific organs (red bone marrow and lower large intestine) are higher. These estimates are in HEDR reports but only for the period 1950 through 1971. In most cases, the farther downstream from Hanford, the lower the exposure.
In order to give a sense of how large a dose 1.5 rem EDE is, a comparison with background radiation is sometimes made. During the same period (1944-1971), an average adult would have received a dose of about 9 rem EDE (whole body) from background radiation. The sources of background radiation include radon, medical procedures, and cosmic rays. Please note that exposure to back-ground radiation may cause adverse health effects.
Representative dose estimates for the river pathway were not calculated for infants and children. For the air pathway, the highest representative dose estimates were for infants and children. Also, dose estimates for the air pathway were reported in a range that was descriptive of the uncertainty in the estimates. The uncertainty range was not reported for the river pathway.
Possible Health Problems
Since the release of the first 19,000 pages of Hanford historical documents in 1986, much has been learned. However, the information available is not enough to form a complete assessment of the impact of Hanford's releases. This section provides information about each of five radionuclides. The same categories of information are presented for each:
1. a general description of the radionuclide;
2. the estimated amount released from Hanford from 1944 to 1971;
3. the possible health effects;
4. the organs estimated to have received the main dose from the Hanford exposures; and,
5. a summary of health studies.
The amounts released, calculated doses and organs receiving the main dose are estimates of HEDR. The five river pathway radionuclides are presented in alphabetical order.
Arsenic-76
Description: The half-life of the radionuclide arsenic-76 is 26.3 hours. It emits beta and gamma radiation. Estimated Amount Released: 2,500,000 curies Possible Health Effects: No studies were found specific to arsenic-76. Organs Receiving Main Dose: Gastrointestinal tract, stomach for infants
Summary of Health Studies
The Network's research has been unable to find any studies on the effects of exposure specific to arsenic-76. Chemically, arsenic, in sufficient concentrations, is a poison and can cause cancer. Chronic exposure to arsenic can cause the following cancers: lung, skin, and stomach (from the chemical toxicity).
Neptunium-239
Description: Neptunium-239 has a half-life of 2.4 days. It emits beta and gamma radiation. Neptunium-239 decays into plutonium-239 which has a half-life of 24,000 years and emits alpha radiation. The amount of neptunium-239 released to the Columbia River decayed to about 1.7 curies of plutonium-239. Estimated Amount Released: 6,300,000 curies Possible Health Effects: Bone cancer Organ Receiving Main Dose: Gastrointestinal tract
Summary of Health Studies
Most of the neptunium that is retained in the body deposits in the bones. Some is also retained in the liver. Several studies report "relatively high concentrations" of neptunium in adrenal glands of laboratory animals.
No health effects specific to exposure from neptunium "have been observed" in human beings. Roy C. Thompson, Biology Department of Battelle Pacific Northwest Laboratory in Richland, conducted an extensive review of studies involving neptunium. This review included Russian studies that found an increase in the number of bone tumors in animals receiving bone doses as low as a few rad. Thompson concluded that "there can be little doubt" that neptunium can cause cancer in bone.
In 1984, a team of German scientists reported preliminary results of an experiment with mice designed to measure the combined effect of having neptunium-239 deposit in bone and decay into plutonium-239. These initial results found evidence that the buildup of plutonium-239 (as the neptunium decayed) increased the number of bone tumors compared to those expected from exposure to neptunium alone.
Phosphorus-32
Description: Phosphorus-32 has a half-life of 14.3 days. It emits beta radiation. Biologically, nonradioactive phosphorus is vital to living things because it enables the transfer of energy in metabolism. It is also an important component in bones. Estimated Amount Released: 230,000 curies Possible Health Effects: Bone cancer, leukemia
Organ Receiving Main Dose: Red bone marrow
Summary of Health Studies
Once inside the body, phosphorus concentrates in the bone. In experiments on rats, phosphorus-32 was found to be "potent" in causing bone cancer.
Based on studies of human patients with polycythemia vera treated with phosphorus-32, there may be an "increased incidence of leukemia." A review article of several studies of people with the same blood disease who were followed until death reported that of those treated with phosphorus-32, 16 percent had developed acute leukemia compared with only 1.6 percent of those not treated.
Sodium-24
Description: Sodium-24 has a half-life of 15 hours, the shortest half-life of the five radionuclides. It emits beta and gamma radiation.
Estimated Amount Released: 12,000,000 curies
Possible Health Effects: No studies were found specific to sodium-24.
Organ Receiving Main Dose: Stomach
Summary of Health Studies
The Network's research has been unable to find any studies on the effects of exposure specific to sodium-24.
Zinc-65
Description: Zinc-65 has a half-life of 245 days, the longest half-life of the five radionuclides. It emits beta and gamma radiation. Biologically, nonradioactive zinc is needed. "Too little zinc in the diet can lead to poor health, reproductive problems, and lowered ability to resist disease." Estimated Amount Released: 490,000 curies Possible Health Effects: Damage to enzymes and hormones
Organ Receiving Main Dose: Whole body
Summary of Health Studies
The principal health effect of zinc-65 is from the radiation exposure. If zinc-65 decays into copper while it is in an enzyme in the body, it can possibly have "drastic consequences." One consequence is that exposure to zinc-65 might lead to the formation of autoantibodies. Evidence for this comes from a study on rabbits.
Zinc also readily concentrates in the prostate when administered intravenously Because of this, radioactive zinc may be a factor in prostate cancer
Summary
To conclude, we know that Hanford's plutonium production did cause extensive contamination of the Columbia River and parts of the Pacific Ocean along the coasts of Washington and Oregon. Fish and other wildlife using these waters were exposed to radioactive materials and other kinds of pollution. People using the waters and the aquatic resources were also exposed to measurable levels of radiation.
What remains uncertain is if and how the radiation released into the Columbia River affected human health. Many people have asked the Network questions about whether their exposure to the radioactive contamination in the Columbia River harmed their health. Unfortunately, there is not enough information to answer their questions.
Unresolved Issues
During the preparation of this report, the technical reviewers raised several points that could not be resolved.
David C. Kocher, Ph.D., was concerned that the presentation of the risk of possible health effects of the five radionuclides was incomplete. Readers should understand that, given the low dose estimates of HEDR, "there is no reason to believe that there was an observable increase in health effects in nearby residents due to releases to the river." Scientists are not now able to observe (or measure) health effects due to exposure to background radiation. Since the dose estimates for the river pathway are lower than background, scientists could not measure "health effects even if they existed, because the effects would be substantially less than those caused by natural background." Kocher is with the Health Sciences Research Division of Oak Ridge National Laboratory in Tennessee.
Norm Buske, M.S., was mainly concerned that possible health effects could not be "reliably appraised until Hanford's major releases have been identified." His assessment is that Hanford's dose reconstruction work has probably overlooked important radiological releases to the Columbia River. Buske suggested that the significance of these releases was "probably greater than anything yet reported" by HEDR. He asserted that HEDR should have included other radionuclides, such as chromium-51 and iron-59, in the dose calculations. Buske has presented his concerns to Hanford officials and is awaiting a response. He has a degree in oceanography and has done research on Hanford radioactive releases and the Columbia River over the last ten years.
Greg deBruler served as the public representative on this report's Technical Review Panel. One of his major concerns is the dose estimates used in this report. "There is enough scientific uncertainty with HEDR that the representative dose estimates should not be treated as if they were scientifically proven facts. The HEDR dose estimates could be off by orders of magnitude of ten or more." DeBruler reminds us of the statement in an HHIN document: "The basic assumption of radiation protection standards is that any exposure to radiation poses a health risk." The review of this document does not reflect all of the comments or concerns he submitted. DeBruler is a technical consultant to Columbia River United, a nonprofit organization based in Hood River, Oregon.
NOTES
1. Oregon Health Division, Radiation Protection Services. Environmental Radiological Surveillance Report on Oregon Surface Waters, 1961-1993. Dec. 1994, p. 1.
2. Walters WH, et al. Literature and Data Review for the Surface-Water Pathway: Columbia River and Adjacent Coastal Areas. PNL-8083, Battelle: April 1992, p. 5.5.
3. For further reading on radiation trapped in sediments, see D Wells, Special Report: Radioactivity in Columbia River Sediments and Their Health Effects. Washington Department of Health, Division of Radiation Protection; Mar. 1994.
4. Although the amounts are much smaller, radioactive material continues to enter the Columbia River from Hanford's contaminated groundwater. This publication covers only the years 1944-1972, as directed by the Network's mandate.
5. Farris WT, et al. Columbia River Pathway Dosimetry Report, 1944-1992. PNWD-2227; July 1994, p. 4.4.
6. Radiation Aspects for River Navigation Through Hanford Project. HW-47152; Dec. 7, 1956, p. 2.
7. For additional information, see Hanf RW, et al. Radioactive Contamination of Fish, Shellfish, and Waterfowl Exposed to Hanford Effluents: Annual Summaries, 1945-1972. PNWD-1986; July 1992.
8. Junkins RL, et al. Evaluation of Radiological Conditions in the Vicinity of Hanford for 1959. HW-64371. Also "Quarterly Progress Report: October-December 1959." HW-63643; pp. 19-20.
9. Corley JP. Environmental Surveillance at Hanford for CY-1970. BNWL-1669; Sept. 1973, pp. 3, 35. Due to changes in how doses are calculated, it was not possible to make a comparison with current standards.
10. Becker CD. Aquatic Bioenvironmental Studies: The Hanford Experience, 1944-1984. Studies in Environmental Science, Volume 39. Amsterdam: Elsevier, 1990, pp. 96-97, 100, 110. Becker was in the Geosciences Department of the Pacific Northwest Laboratory at Hanford which is operated by Battelle.
11. Becker CD. p. 175.
12. Dauble DD, et al. Radionuclide Concentrations in White Sturgeon from the Columbia River. PNL-8221, Rev. 1; November 1993, p. 18.
13. Becker CD. p. 110.
14. Parker earned a Masters of Science in physics from the University of Manchester in England (1931). He then worked on using radiation to treat cancer in both England and the United States. For the four years immediately prior to World War II, Parker worked under Simeon Cantril at the Swedish Hospital Tumor Institute in Seattle. During the Manhattan Project, Parker worked to develop radiation protection procedures at Chicago, Oak Ridge, and Hanford.
15. Parker HM. Columbia River Situation-A Semi-Technical Review. HW-32809; August 19, 1954.
16. Thomas J. Atomic Deception: Oh, What a Tangled Web! HEAL Perspective. Summer/Fall 1992; (10-11): p. 7.
17. US Public Health Service. Evaluation of Pollutional Effects of Effluents from Hanford Works. May 13, 1964.
18. Wells D. Special Report: Radioactivity in Columbia River Sediments and Their Health Effects. Washington Department of Health, Division of Radiation Protection. Mar. 1994; p. 41.
19. CRITFC (Columbia River Inter-Tribal Fish Commission). A Fish Consumption Survey of the Umatilla, Nez Perce, Yakama, and Warm Springs Tribes of the Columbia River Basin. CRITFC Technical Report No. 94-3, October 1994; p. 59.
20. Farris WT, et al. Columbia River Pathway Dosimetry Report, 1944-1992. PNWD-2227; July 1994, p. 4.8.
21. Thompson RC. Neptunium-The Neglected Actinide: A Review of the Biological and Environmental Literature. Radiation Research. April 1982; 90: p. 1
22. Thompson. p. 21.
23. Thompson. p. 24.
24. M�ller WA, Sch�ffer EH, Linzner U, Luz A. Incorporation Experiments with Combined Application of Different Bone Seekers. Radiation Environment Biophysics. 1984; 23 (2): p. 115. The scientists were from Abteilung f�r Pathologie, Gesellschaft f�r Strahlen- und Umweltforschung, Neuherberg, Germany (in association with EURATOM).
25. Goldman, M. Experimental Carcinogenesis in the Skeleton. In Radiation Carcinogenesis, AC Upton, RE Albert, FJ Burns and RE Shore, eds. 1986; p. 220. (Dr. Goldman is from the Laboratory for Energy-Related Health Research, University of California-Davis.)
26. Visfeldt J, Jensen G, Hippe E. On Thorotrast Leucaemia: Evolution of Clone of Bone Marrow Cells with Radiation-Induced Chromosome Aberrations. ACTA Pathologica et Microbiologica Scandinavica. July 1975; 83 (4): p. 377. (Visfeldt is with the University Institute of Pathological Anatomy in Copenhagen, Denmark. Jensen is with the Institute of Pathology, Frederiksberg Hospital in Copenhagen. Hippe is with the Medical Department C at the Bispebjerg Hospital, also in Copenhagen.)
27. Rothstein G, Wintrobe MM. Preleukemia. Advances in Internal Medicine. 1975; 20: p. 367. (Both authors were with the Department of Internal Medicine at the University of Utah, College of Medicine in Salt Lake City.)
28.
29. Schulte HF. Los Alamos Scientific Laboratory. Book review of The Toxicology of Radioactive Substances, Volume 5: Zinc-65. Health Physics. September 1971; 21 (3): p. 481.
30. Filatov PP. The Effect of Chronic Exposure to Radioactive Zinc on Antibody Formation. The Toxicology of Radioactive Substances, Volume 5: Zinc-65. AA Letavet and EB Kurlyandskaya, eds. Oxford: Pergamon, 1970, pp. 138ff.
31. Cottrall MF. Medical Research and Auger Cascades (letter). The Lancet. Oct. 26, 1985; 2 (8461), pp. 942-943. (Cottrall was with the Academic Department of Medical Physics at the Royal Free Hospital School of Medicine in London.)
32. Prout GR, et al. Radioactive Zinc in the Prostate: Some Factors Influencing Concentrations in Dogs and Men. JAMA. April 11, 1959; 169 (15): pp. 1703-1710. Prout was with the Urologic Service of the Sloan-Kettering Institute.
33 Hilson A. Prostatic Cancer and Radionuclides: Evidence Implicates Zinc-65 (letter). BMJ. January 22, 1994; 308: p. 268. (Hilson is in the Department of Nuclear Medicine at London's Royal Free Hospital.)
Related Reading Available from HHIN
HEDR Technical Steering Panel, Representative Hanford Radiation Dose Estimates, April 21, 1994, Revision 1
HHIN, Potential Health Problems from Exposure to Selected Radionuclides (Released to the Air)
HHIN, Radioactivity in the Body

Many callers to the Hanford Health Information Lines have questions and concerns about the release of plutonium and other radioactive materials from Hanford. Some downwinders have health problems and believe that they are, or might be, related to Hanford. The personal perspectives within this monograph are offered to help readers understand these experiences and concerns. This personal perspective of a member of the Confederated Tribes of the Umatilla Indian Reservation can help readers understand the experiences and concerns of Tribal members.
"I first went to Celilo Falls at age eleven in the early 1940s. Here I caught and handled a lot of salmon during the span of three fall fisheries. First I was a fish buyer for my uncle and secondly, an enterprising fisherman. Since I had no scaffold of my own to fish, I moved around to available places and had a lot of fun. My family wasn't dependent upon the fisheries, but we consumed a lot of salmon.
"To the best of my knowledge, there have been little ill effects to myself or immediate family from Hanford's radioactive releases into the Columbia River. However, the river is very sick. There are many questions from Tribal members who have spent more of their time around the river, about the deaths of their relatives. They have many unanswered questions about what happened at Hanford and how it could affect us.
"At this point we don't have any definite answers that say this was a result of something that was released to the water or air from Hanford. All we know about radionuclides is, you can't see them, hear them, smell them, or taste them - but they can affect you."
Name withheld by request
Talking with Patients about Radiation Health Effects: Case Histories and Discussion
OBJECTIVES
After studying this module, the reader will be able to
* List a range of clinical problems reported by downwinders ("Downwinder" is the term often used to describe a person who may have been exposed to radiation because he or she lived "downwind" or "downriver" from the Hanford Nuclear Reservation)
* Identify the concerns and frustrations faced by downwinders who have questions about the possible
relationship between radiation exposure and health problems
* Explain to patients associations between radiation exposure and health care problems
Introduction
Prior to 1986, few people knew about the radiation released from the Hanford Nuclear Reservation from 1944 to 1972. Over the last decade, however, public awareness of Hanford's releases has increased. Today, many health care professionals are seeing patients who have questions and concerns about the significance of their exposure to Hanford's radioactive releases and about the possible link of this exposure to the health problems they may experience.
Exposure to radiation brings with it great uncertainty. Radiation is an invisible contaminant - it is not seen, felt, heard, smelled, or tasted. While acute exposures that result in high whole-body doses of radiation (50 rad or above) will cause certain immediate health effects ranging from mild nausea to death, chronic low whole-body doses have unpredictable health effects that are often medically invisible for long periods of time.
When a person develops an illness or disorder, it is usually not possible to determine whether radiation or other agents caused or contributed to the problem. In spite of these uncertainties, both the provider and patient benefit from open discussions about the possibility of a link between radiation exposure and a downwinder's health problem.
Notes About The Case Histories
The following case histories represent four of the approximately two million people exposed to radiation from Hanford. Some people had more exposure to Hanford's radioactive releases than the people in these case studies, while other people had less exposure.
Each case history was developed by telephone interviews with a downwinder who was identified by the outreach staff of the Hanford Health Information Network. The written description of each case was sent to the downwinder for review. A copy of the case was also given to a health care provider identified by the downwinder for technical review; however, not all providers chose to comment on the cases. Lab work relevant to the downwinder's primary health problems was requested and included in the case history when available.
Each case begins with a residence history and a brief description of lifestyle factors that would have contributed most to the individual's radiation dose from Hanford. This is followed by a summary of health care problems, medications, and family history. There is a discussion of the associations between the kinds of health problems the individual has experienced and current radiation health effects research. Each case history concludes with a synopsis of the person's own reflections which include questions and beliefs about the possible connections between exposure to radiation from Hanford and the person's health.
Case History #1
Hanford-Related Residences
This individual was conceived in Richland, Washington, and born there in January 1949. She lived in Richland until 1952.
Lifestyle Factors
During pregnancy, her mother drank locally produced milk and ate locally grown fruits and vegetables. As an infant, this woman was breast fed for just one week. She is uncertain if she received formula or canned milk in her first year of life. The family bought milk from local dairies which she drank while still in Richland. The family also bought and ate locally grown fruits and vegetables, but did not eat fish from the Columbia River. The family did not use the Columbia River for recreational purposes and drank city water, which, at that time, was not from the Columbia River.
Health Problems
History of Problems
Hypothyroidism: In September 1989, this woman became pregnant for the first and only time. Within days of becoming pregnant she developed a cold which progressed to pneumonia. Although the pneumonia resolved after treatment with antibiotics, she feels she never really got well. Her pregnancy was confirmed two months after conception, but she miscarried two days later. She continued to feel tired all the time and eventually went to an endocrinologist. A goiter the size of a golf ball was discovered in March 1990. She was diagnosed with hypothyroidism and has taken medication since that time. She had infertility problems and wonders if they were related to undiagnosed thyroid disease.
Immune System Dysfunction: As a high school student she had mononucleosis and missed six months of school. During the time this individual was ill with pneumonia in 1989, she was diagnosed with immune system dysfunction. She has been told by different physicians that she has systemic lupus erythematosus, fibromyalgia, and/or chronic fatigue syndrome. These varying diagnoses are representative of her more general immune system dysfunction. She has had a positive ANA, but a negative anti-DNA and lupus panel.
At one time she took prednisone and other medications for her immune system disorders. She discontinued the medications after experiencing side effects. By limiting her activity and monitoring her diet she feels better. Nonetheless, she experiences episodes of illness which she describes as feeling like a truck hit her: Her limbs feel like lead, she has crushing fatigue, and getting up is difficult. These episodes can last days to weeks.
Past History
1969, 1981, 1989: Pneumonia
1989: Osteoarthritis of the spine
1989: Miscarriage
1991: Interstitial cystitis with recurrent flare-ups
Medications
Levothyroxine sodium (Synthroid) .125 mg qd
Liothyronine sodium (Cytomel) .10 mg qd
Use of both medications began in March 1990. Health Habits and Exposures
Cigarette smoking: Never.
Alcohol use: Drinks wine on weekends, two to three glasses. Rare martini. Drank more in early 20s.
Pesticide exposure: None.
Occupational exposure: None. Other radiation exposure:
Radionuclide scan for evaluating thyroid gland.
Family History
Mother: Alive and well.
Father: Had a thyroidectomy in 1953 for thyroid nodules.
Sister: Has chronic fatigue syndrome and endometriosis. She is ten years younger than this patient and never lived in the Hanford area.
Discussion
During the years this downwinder resided in the Hanford area, 1949-1952, air releases of iodine-131 diminished from the high levels released from 1944 to 1947. Nonetheless, there were periodic high releases (such as the release known as the Green Run on December 2 and 3, 1949, and during the period from April to July, 1951).
This downwinder had an in utero exposure to radiation through her mother's consumption of local milk and produce. The downwinder herself also consumed local milk and produce during her years of residence in the Hanford area.
Laboratory Data February 1990 Results Reference Range T3U 26.4 26-36 T4(RIA) 9.5 5.0-13.4 TSH 1.1 0.9-4.6 Antithyroid microsomal AB less than 20 25 or less Anti-thyroglobulin AB less than 10 20 or less ANA (FANA) Positive Anti-DNA Negative March 1990 Radionuclide Scan (iodine-123 and Technetium 99): Slightly low uptake with normal sized and uniformly labeled gland, consistent with mild hypothyroidism. April 1993 Results Reference Range T4 2.0 0.71-1.85 TSH 0.3 0.9-4.6 Consumption of locally produced milk is the main way that people received doses of iodine-131 from Hanford's radioactive releases. This is also a route of exposure to other radionuclides. Consumption of locally grown fruits and vegetables is the next most significant route for receiving doses of iodine-131.
Large doses (greater than 350 rad) of iodine-131 or external radiation can produce hypothyroidism by destroying thyroid tissue. Studies of humans exposed to a wide range of doses, primarily from external radiation, have shown conflicting results ranging from no effect to increases in autoimmune thyroiditis, Graves' disease, adenomatous goiter, and nodules without specific diagnoses. There is still controversy over whether radiation can cause these diseases and, if so, at what doses and by what mechanisms.
Thyroid blood tests on this downwinder were negative for thyroid antibodies, indicating that this is not a case of autoimmune hypothyroidism, a thyroid disease that one study has associated with exposure to radiation from the atomic bomb in Nagasaki, Japan.1 It is unlikely that this patient's hypothyroidism was related to her pregnancy which ended in the first trimester. However, thyroid dysfunction, including toxic nodular goiter, thyroiditis, and Graves' disease, are known to occur during pregnancy.
There is little research on people exposed to low doses of radiation and its effects on their immune systems. High doses of radiation weaken the immune system. Although low-dose radiation has been shown to cause mutations and chromosomal aberrations in the lymphocytes of children and adults, its effect on immune function is not clear. At this time, there is no known association between exposure to radiation and fibromyalgia, chronic fatigue syndrome, or systemic lupus erythematosus.
Personal Reflections on Hanford
She is concerned that in utero exposure to radiation and living near Hanford for the first three years of life contributed to her illnesses, particularly her thyroid disease. She recognizes that her sister, who never lived in the Hanford area, has some similar problems, notably chronic fatigue syndrome. She wonders, however, if her parents' radiation exposure contributed to both her and her sister's illnesses.
Case History #2
Hanford-Related Residences
This individual was born August 19, 1945. She lived in various places until her family settled in the Hanford area in 1953. Then, from 1953 to 1963, she lived across the Columbia River from Hanford near Ringold. Between 1963 and 1965 she lived in Pasco, Washington. She lived in eastern Oregon from 1967 to 1969. Lifestyle Factors
From 1953 to 1963, this person lived with her family on a farm. She drank an average of one-half gallon of milk a day from the farm's cows. The family grew most of its vegetables and some fruit and ate other locally grown produce. The garden and the farm's crops were irrigated with Columbia River water. Cattle raised for beef were fed these crops. The family also raised and ate pigs, chickens, and rabbits.
For three years before running water was available, she remembers swimming in the irrigation ditches and ponds as a way of bathing. The family's drinking water was always from a well. The family ate small quantities of Columbia River fish.
Health Problems
History of the Problems
Fibromyalgia: The patient remembers having symptoms of fibromyalgia as far back as 1961. She has chronic pain from her neck to her sacrum. Myelograms failed to provide a definitive diagnosis. She started on pain medication in 1971 and attained some relief. Her primary provider referred her to a rheumatologist for evaluation and, in 1976, she was diagnosed as having fibromyalgia.
Deterioration of the vertebrae: She had two neck fusions using bone grafts in 1984. She had right thoracic outlet surgery in 1985 and an anterior fusion with a titanium plate in 1988. The anterior fusion was repeated later that year. She has limitations on bending her neck and has chronic pain there and in her shoulders, as well.
Chronic Fatigue Syndrome: Initially diagnosed as having an infection with Epstein-Barr virus in the late 1980s, she was diagnosed in 1990 with chronic fatigue syndrome.
Past History
1980: Duodenal ulcer secondary to anti-inflammatory drug use
1993: Bleeding of duodenal ulcer with blood transfusion
Hepatitis B contracted from blood transfusion
Osteoarthritis of the hands and feet for eight to ten years
Cyst removed from right breast
Cysts (two) removed from lower back
Health Habits and Exposures
Cigarette smoking: Began at age twenty-six when pain was difficult to cope with and stopped ten years later. Smoked one pack per day on average.
Alcohol use: Occasional.
Pesticide exposure: Some pesticides were used in the area but not on her family's farm.
Occupational exposures: None.
Other radiation exposures: She may have received an exposure in utero to fallout from the Trinity test of the first nuclear device in July 1945. Her parents lived in Clovis, New Mexico, about 250 miles northeast of the Trinity site.
Family History
Mother: Osteoarthritis; fibromyalgia diagnosed within the last ten years.
Father: Multiple sclerosis ten to twelve years.
Daughter: Born in 1966; fibromyalgia.
Son: Stillborn in 1969.
Son: Born in 1970, two months premature with immune system and respiratory problems.
Discussion
This downwinder's years of residence in the Hanford area coincide with the years of highest releases from Hanford to the Columbia River. Releases to the air were lower after 1948, although there were episodic releases of concern through 1957. According to the Hanford Environmental Dose Reconstruction Project (HEDR), Ringold was in the area which received the highest concentrations of Hanford's iodine-131 emissions. Ringold was usually downwind from Hanford.
The consumption of milk from a family cow is the exposure that would result in the highest dose of iodine-131 from the radioactive releases from Hanford. However, this woman's period of Hanford-area residence was during a time of comparatively small air releases. The consumption of locally grown fruits and vegetables is the second most significant pathway for exposure to iodine-131.
HEDR estimated that the contribution to dose from eating crops irrigated by Columbia River water was so small that dose estimates were not calculated for this pathway. If the irrigation water in which she swam for three years came from the Columbia River below Hanford, then exposure was from external whole-body radiation. HEDR estimated that this external whole-body exposure made a small contribution to dose. HEDR estimates a dose less than 5 mrem EDE for the years 1956-1965 for a typical representative individual living in Pasco, Washington. Drinking radioactively contaminated water and eating radioactively contaminated fish were the main sources of dose from the Columbia River. (HEDR estimates a maximum dose of 4 rem EDE for the years from 1944-1971.)
This downwinder's primary health problems are fibromyalgia and chronic fatigue syndrome. These are considered to be immune system disorders of unknown etiology. There is little research on people exposed to low doses of radiation and its effects on their immune systems. High, acute doses of radiation weaken the immune system. Although low-dose radiation has been shown to cause mutations and chromosomal aberrations in the lymphocytes of children and adults, its effect on immune function is not clear. Except for evidence of a relation between radiation exposure and autoimmune thyroiditus, no association has been made between such changes and immune disease in humans. At this time, there is no known association between exposure to radiation and fibromyalgia or chronic fatigue syndrome.
Personal Reflections On Hanford
This person feels she has always had poor health, even as a child. When she lived near Hanford, she recalls concerns about Hanford being voiced by neighbors. She became aware of the radioactive releases from Hanford in 1987 or 1988. She has always questioned why she was so sick. Her father's illness made her wonder about connection to Hanford even more. She was referred from one doctor to another. One doctor decided her pain was due to depression and referred her to a psychotherapist. She felt her depression was due to pain. Now she looks at Hanford as a possible source of her health problems and those of her family.
Case History #3
Hanford-Related Residences
This individual was born on December 5, 1944, in Spokane, Washington, where she lived for five years. She then moved to a small town southeast of Spokane where she has lived ever since.
Lifestyle Factors
As a baby, this person had a lactose intolerance. She was given specially prepared milk that was either canned or store-bought. Her family moved to a farm when she was five and kept a cow in the yard. She drank this cow's milk with each meal. The cow's milk was also consumed in home-made ice cream and cooked foods. Her mother grew most of their vegetables and berries. When they moved to the farm, they picked fruit in the area. The family also produced its own meat, eggs, dairy products, pigs, and chickens, along with some wheat.
The family did not eat fish from the Columbia River, drink its water or use the river for recreational purposes.
Health Problems
History of the Present Problems
Thyroid Disease: This woman says her symptoms of thyroid disease began when she was in the hospital after delivering her daughter in January 1966. She had heat intolerance which progressed over the course of months. She experienced excessive thirst, felt very stressed, and had heart palpitations. Her family physician tested her in mid-1966 and diagnosed hyperthyroidism. She took medication four times a day for at least a year. She is unsure of the name but it was a small white pill. Finally, she was tapered off the medication and had no problems until 1983.
While singing in 1983, she felt like she was getting laryngitis. She initially thought it was related to a cold, but it persisted over time. One day she noticed a mass in her neck and felt a lump the size of a pea. She had no other symptoms.
At the time, her TSH was very high. A radionuclide scan indicated decreased activity in the right thyroid lobe. Results of a needle biopsy indicated cancer. Pathology of the tumor revealed papillary carcinoma, chronic thyroiditis, and Hashimoto's thyroiditis. She underwent surgical removal of all but a portion of the left side of the thyroid.
Past History
1978: Cholecystectomy
1988: Hysterectomy and right salpingo-oophorectomy
1994: Esophageal reflux
Medication
Levothyroxine sodium (Synthroid) .2 mg qd
Health Habits and Exposures
Cigarette smoking: Never smoked.
Alcohol use: None.
Pesticide exposure: There was some DDT spraying in the area and possibly a limited amount on the family acreage. Their farm was at a higher elevation than many other farms so the water source and fields were above where most spraying would have occurred.
Occupational exposures: None.
Other radiation exposures: Radionuclide scan; routine X-rays.
Family History
Mother: Alive and well.
Father: Died in a car accident.
Brother: Hiatal hernia and gall bladder disease.
Daughter: Born 1966, is well.
Daughter: Born in 1970, diagnosed with Hashimoto's thyroiditis at age seventeen or eighteen.
Aunt: Died from breast cancer in the past year. Lived southwest of Spokane.
Laboratory Data December 1983 Pathology Report from Thyroid Surgery: Papillary carcinoma of the thyroid, right lobe; chronic thyroiditis, Hashimoto's type; thyroiditis of the left lobe. April 1990 Pathology Report from Hysterectomy: Late proliferative phase endometrium; adenomyosis uteri, marked; benign leiomyomata; chronic cystic cervicitis with focal squamous metaplasia of the distal endocervical canal; small follicular cysts of the right ovary; parovarian cyst. Aunt: Diagnosed with lupus within the last six to eight years. Lived in the Spokane area.
Discussion
The Spokane area is considered to be downwind of Hanford and routinely received deposition of airborne releases. Her residence in this area includes the years of the largest air releases from Hanford. While the airborne releases from Hanford declined significantly after 1947, milk from a backyard cow was the pathway through which persons received the highest doses of iodine-131.
Consumption of locally grown fruits and vegetables was the second most important way persons were exposed to iodine-131. This person consumed these foods during the years of the largest air releases from Hanford.
A likely diagnosis of this patient's hyperthyroidism in 1966 is Graves' disease, which accounts for 10 percent of all post-partum cases of hyper-thyroidism. It is possible that the hyperthyroidism was caused by an adenoma, although this is a rare condition. In 1983, this patient was diagnosed with thyroid cancer. This is seen in some people with Graves' disease. Both Graves' disease and tumors are associated with exposure to radiation.
As discussed in the introduction, thyroid cancer and benign neoplasms are associated with exposure to iodine-131. This downwinder had papillary carcinoma of the thyroid. In a study conducted between 1965 and 1986 of 2,473 Nevada Test Site downwinders, fifty-six had thyroid nodules. Of these, thirty-eight had non-neoplastic nodules, eleven had benign neoplasms, one had both papillary carcinoma and a non-neoplastic nodule, and eight subjects had papillary carcinomas. Despite the small number of cases of papillary carcinoma, the dose-response trend achieved marginal statistical significance.2
Radioactive fallout from a nuclear weapons test in 1954 exposed Marshall Islanders to external gamma radiation, iodine-131, and three other forms of radioactive iodine. They experienced an increased rate of hypothyroidism and both malignant and benign thyroid tumors. It is difficult to say whether it was iodine-131 or the radioactive iodines alone that caused the thyroid problems because the Marshall Islanders also received gamma radiation.
The pathology report included in this case history documents the presence of both thyroiditis and Hashimoto's thyroiditis. Thyroiditis may result from large doses of external radiation. The radiation may be indirect, as when children received X-ray therapy in the past for skin and scalp diseases. Direct external radiation to the area of the thyroid gland can also cause thyroiditis. There is nothing in this person's history that indicates large doses of external radiation.
Hashimoto's thyroiditis involves autoimmune factors. The lab data available do not indicate that evaluation for autoimmune thyroiditis was conducted. This would be interesting information in view of the 1994 report by a team of Japanese scientists. They found an increased risk for antibody-positive spontaneous hypothyroidism (a form of autoimmune hypothyroidism) among survivors of the atomic bombing of Nagasaki who received external exposure to radiation. Patients with Hashimoto's thyroiditis are commonly antibody positive. In the Hanford situation, nearly all of the dose was internal. The Hanford Thyroid Disease Study (HTDS) is including an assessment of autoimmune thyroid disease in its study, as well as an assessment of hyperthyroidism and thyroid neoplasms.
Personal Reflections on Hanford
She is concerned that her thyroid disease is related to the radioactive releases from Hanford. She has been surprised by the information she has read about Hanford and believes that a large number of people have died of cancer in the area where she has lived for thirty-one years. She wonders if these deaths are related to Hanford.
Case History #4
Hanford-Related Residences
This individual was born in January 1949 in Sunnyside, Washington. She resided with her family in Grandview, Washington, from 1949 until 1952. Between 1952 and 1956, she lived in Coeur d'Alene, Idaho. She moved to Othello, Washington, in 1956, where she lived until 1968.
Lifestyle Factors
This person's milk source was either a backyard cow or milk bought from a local farmer. She recalls drinking large quantities of milk, but cannot specify how much. Her family always had a garden and ate other local produce which included lots of leafy green vegetables.
She recalls eating fish her father caught in lakes and in the Columbia River (more from lakes than the river). She cannot recall the type or quantity of fish they consumed. Her drinking water was either city water or well water. She did not use the Columbia River for recreational purposes.
Health Problems
History of the Problems
Thyroid Disease: In the spring of 1966, she saw a doctor when she found a lump in her neck and had trouble swallowing. She was diagnosed as having tonsillitis. She returned to the physician in July of that year when the lump got bigger and she gained weight. Although the doctor assessed her clinically as being hypothyroid, tests indicated she had a toxic goiter and was hyperthyroid.
From July 1966 to September 1966, she received medical treatment and when medication failed, underwent surgical removal of 90 percent of her thyroid. She required no thyroid medication following surgery.
In 1974, she developed hyperthyroidism again. She was quite surprised given that most of her thyroid gland had been removed. She was treated medically for four years until 1978. At that time, she received iodine-131 to destroy the remaining thyroid tissue. A physician at a military hospital where she sometimes receives treatment recently told her she has Graves' disease. Despite taking thyroid medication, she continues to be fatigued and has cold sensitivity.
Infertility: This individual's experience with infertility may have been secondary to her thyroid disease. She used birth control for only one month between her first and second pregnancies, nine years apart. She became pregnant after treatment with iodine-131 for thyroid disease. Past History
1967: Undiagnosed gait disturbance
1986: Vasculitis of the left brain MRI revealed three earlier "mini-strokes"
Current Medication
Levothyroxine sodium (Synthroid) .15 mg daily.
Health Habits and Exposures
Cigarette smoking: None.
Alcohol use: Occasional.
Pesticide exposure: Area crops were dusted with pesticides. Her father grew wheat and alfalfa and she played in the fields.
Occupational exposure: None.
Other radiation exposure: Radionuclide scan for diagnosis of thyroid disease in 1970s and iodine-131 treatment in 1978. Also, her mother spent part of her pregnancy in the Hanford area after moving from a mid-western state, so this woman received some in utero exposure.
Family History
Father: Deceased; had hypertension and heart problems.
Mother: Alive and has hypotension.
Sister: Had thyroid surgery with a portion of the gland removed five years after the subject's surgery (sister is older by fourteen months and was born in a mid-western state). Also on thyroid medication following surgery.
Brother: Aneurysm, age twenty-nine.
aughter: Born 1971 and has mild scoliosis.
Son: Born 1980 with a meningomyelocele, died at twenty-two days old.
Daughter: Born 1983 with anencephaly at thirty-two weeks gestation, deceased at one and one-half hours.
Discussion
This downwinder resided in the Hanford area after the period of the largest air releases from December 1944 through 1947. Air releases, however, continued to be a concern through 1957, with intermittent high releases such as the Green Run experiment on December 2 and 3, 1949. Sunnyside and Grandview were usually upwind from Hanford which would result in a lower exposure to radiation compared to residents of communities equidistant, but downwind, of the Hanford Site.
This downwinder drank milk from a backyard cow, the most important source of a dose of iodine-131. Locally grown vegetables and fruit, which she also consumed, were the second most important source of exposure to iodine-131.
The late 1950s and early 1960s were the years of peak releases to the Columbia River. Eating fish from the Columbia was one of the two most important ways that people could be exposed to radioactivity from this source. This person did not drink Columbia River water, the other important exposure route.
Radiation-induced thyroid disease is generally considered to encompass hypothyroidism and thyroid neoplasia. Hyperthyroidism has been reported in persons with external exposure to ionizing radiation and there is no reason to believe that exposure to iodine-131 would not produce similar effects. Thyroid nodules, which can be caused by external radiation or iodine-131, can cause hyperthyroidism. No laboratory data were obtained for this downwinder, so it is unknown if she had nodules at the time of her thyroidectomy in 1966, or when she had recurrent hyperthyroidism in the late 1970s. HTDS will assess the relationship between iodine-131 doses to the thyroid and thyroid diseases including hyperthyroidism.
Sever et al 3reported an association between neural tube defects and the paternal pre-conception dose of Hanford workers. This effect was observed in children whose fathers received low doses (10 rem or less) of external whole-body radiation while working at Hanford.
This study covered the years 1957-1980.
Sever et al 4 also conducted a study of neural tube defects in Washington's Benton and Franklin counties (near Hanford) between 1968 and 1980 and reported a higher-than-expected rate of neural tube defects. The county rates were compared to rates from Washington, Oregon, and Idaho. This study has many limitations, including the years examined and the way in which doses were estimated. The period studied did not include the time of highest releases to the air.
Currently, Sever is the principal investigator of a case-control study of childhood leukemia and the relationship between parental preconception occupational exposure to radiation. Hanford is one of the sites included in the study.
Personal Reflections on Hanford
This woman considers it very likely that her thyroid disease is related to her exposure to the radioactive releases from Hanford. She is quite concerned about the genetic effects of the radioactive releases because each of her three children had some sort of neural tube defect ranging from mild to severe.
She received genetic counseling after her second pregnancy and was advised that there was a five percent chance another child would have a neural tube defect. She was also advised to take vitamins and folic acid before becoming pregnant again, which she did. She and her husband adopted a child after her third pregnancy rather than risk having another child with neural tube problems. Her daughter has a child who appears to be well, which greatly relieved her concerns about passing on this problem to yet another generation.
Summary
These case histories illustrate the residence background and lifestyle factors that help determine the radiation doses from Hanford for four individuals who were exposed to Hanford's radioactive releases via the air and river pathways. Each downwinder lived in various parts of HEDR's study area during different years of Hanford's operations. Each has a particular set of lifestyle factors that affect the radiation dose received. Each case demonstrates a different set of health problems and concerns. To date, there are only a few studies that have been conducted on the relationship between radiation from Hanford and health effects in the general public. None of these has produced clear-cut results. However, according to the International Commission on Radiological Protection, the basic assumption of radiation protection is that any exposure to radiation poses a health risk. One study of Hanford now underway may add to our knowledge of the health effects of Hanford's radioactive releases.
HTDS is investigating:
Whether thyroid morbidity (including, but not limited to, hypothyroidism, benign neoplasia, and malignant neoplasia) is increased among persons exposed to releases of radioactive iodine from the Hanford Nuclear Site between 1944 and 1957, and who received radiation doses to the thyroid as a result, relative to persons who received a very low or negligible radiation dose to the thyroid from Hanford. If an effect is detected, the study is designed to further determine in what way the increase in thyroid morbidity is related to the dose of radiation received (i.e., the characteristics of any dose-response relationship).5
A team of investigators at the Fred Hutchinson Cancer Research Center is conducting the study under a contract with the Centers for Disease Control and Prevention. The study is scheduled to be completed in 1998.
Recent findings from studies of other populations suggest relationships between exposure to iodine-131 and thyroid disease. An article published in the August 3, 1994, issue of the Journal of the American Medical Association reports an increase in the number of Japanese atomic bomb survivors with autoimmune thyroiditis. This study is the first to detect the link between autoimmune disease and external radiation exposure among the atomic bomb survivors.
The rate of thyroid cancer has increased dramatically in the areas most affected by the 1986 Chernobyl nuclear accident.6 Before the 1986 accident, the rate of thyroid cancer in the areas around Chernobyl was similar to rates in other parts of the world. Now the rate is up to 200 times higher than before the Chernobyl accident. The major contribution to thyroid dose in this population is from iodine-131. There are still many unanswered questions about the health effects of the radioactive releases from Hanford. The preceding case histories include Hanford downwinders who have been diagnosed with diseases that have been associated with radiation exposure in other populations. The case histories also include people diagnosed with diseases such as fibromyalgia and chronic fatigue syndrome which have not yet been linked to radiation. The cases also demonstrate how some people encounter problems or delays in receiving a proper diagnosis for thyroid disease. Screening and Assessment Guidelines
This monograph includes recommendations for screening and assessment of thyroid disease in people exposed to Hanford's releases. Briefly, these recommendations include the following:
* Complete history with attention to residence history, radiation exposure, and prior thyroid disease
* Complete physical examination with thyroid examination
* Laboratory to include T3 and TSH
* Thyroid nuclear scan or ultrasound scan if a thyroid problem is clinically suspected
* Fine needle aspiration biopsy of a thyroid nodule
* For individuals with normal evaluation, re-screen yearly or less often in specific cases Follow-up of abnormal screening
At this time, there are no other recommendations for screening and assessment guidelines specific to people exposed to radiation from Hanford. However, routine periodic health maintenance and prevention activities should be conducted. This will minimize the possibility of a disease going undiagnosed and also provide reassurance to people who are well.
Psychological Effects of Invisible Trauma
The psychological effect of an invisible trauma such as exposure to radiation can be devastating. The invisible nature of radiation brings with it a set of concerns that Vyner7 refers to as a typology of uncertainty. Vyner studied atomic veterans (military personnel exposed to the atomic bombings in Japan or atomic bomb tests in the United States). Health care providers often hear Hanford downwinders discuss many of the same uncertainties that Vyner identified in atomic veterans.
The uncertainties relevant to Hanford downwinders are as follows:
1. Previous exposure uncertainty: Whether or not one has been exposed to an invisible contaminant in the past and, if exposed, whether any dose was received.
2. Present exposure uncertainty: Whether or not one is in the process of absorbing invisible contaminants and, if so, what is absorbed.
3. Boundary uncertainty: What are the geographical limits of an invisible exposure?
4. Dose uncertainty: How large a dose a person received is often in question if the person was not monitored (or if there was no technology to conduct monitoring).
5. Significance-of-dose uncertainty: If the dose received is known, whether that dose will result in disease.
6. Latency uncertainty: If there is a known exposure, what amount of time will elapse between exposure and the onset of detectable symptoms or disease?
7. Etiological uncertainty: It is difficult to determine whether a specific disease or disorder was caused by an exposure to the suspected agent.
8. Diagnostic uncertainty: Symptoms that arise after an exposure to an invisible contaminant may be difficult to diagnose as a specific medical problem.
9. Prognostic uncertainty: People experience apprehension about their future health when they believe or know they have been exposed to a toxic agent.
10. Treatment uncertainty: When a diagnosis cannot be made, a provider does not know what type of treatment to recommend.
11. Coping uncertainty: The inability to know what to adapt to or what is the proper adaptation.
12. Financial uncertainty: The question of who may be morally or legally responsible for the financial losses and costs caused by the invisible contaminant. Conclusion
Scientists, health care providers, and downwinders alike have many unanswered questions about how exposure to Hanford's radioactive releases may have affected human health. Some of these questions are now under investigation. Other questions have yet to be explored. Many may never be answered.
Health care professionals who acknowledge downwinder concerns will earn the respect and appreciation of their clients. Acknowledging these concerns, along with providing regular health screening and indicated treatment, will help health care professionals forge good working relationships with downwinders.
References
1. Nagataki S, et al. Thyroid Diseases Among Atomic Bomb Survivors in Nagasaki. JAMA 1994; 272 (5): 364-370.
2. Kerber R, et. al. A Cohort Study of Thyroid Disease in Relation to Fallout from Nuclear Weapons Testing. JAMA 1993; 279(17): 2076-2082.
3. Sever LE, et al. A Case-Control Study of Congenital Malformations and Occupational Exposure to Low-Level Ionizing Radiation. American Journal of Epidemiology 1988;127(2): 226-242.
4. Sever L, et al. The Prevalence at Birth of Congenital Malformations in Communities Near the Hanford Site. American Journal of Epidemiology 1988;127(2): 243-254.
5. Fred Hutchinson Cancer Research Center. Pilot Study Final Report: Executive Summary. January 24, 1995, page VII.
6. British Medical Journal, March 25, 1995, p. 801.
7. Vyner H. 1988. Invisible Trauma: The Psychological Effects of Invisible Environmental Contamination. Lexington, Massachusetts: Lexington Books.
Glossary
ALPHA PARTICLES
Alpha particles are positively charged particles made up of two protons and two neutrons. The particles lose their energy quickly and do not penetrate the surface of the skin if the body is exposed externally. Material containing alpha radioactivity can enter the body through a cut in the skin, by ingestion, or inhalation. Uranium-238 and plutonium-239 are sources of alpha radiation.
BEIR V
The latest National Research Council Committee on Biological Effects of Ionizing Radiations is known as BEIR V. The committee's report is Health Effects of Exposure to Low Levels of Ionizing Radiation.
BETA PARTICLES
Beta particles are fast moving electrons which are negatively charged. Beta radiation can penetrate a few millimeters in human tissue before losing all of its energy. Iodine-131, phosphorus-32, and strontium-90 are all sources of beta radiation.
CURIE
This is a measure of radioactive material. It measures the number of atoms that decay each second. One curie is 37 billion atoms undergoing decay each second. Hanford released an estimated 739,000 curies of iodine-131 from 1944 to 1972. In contrast, the 1979 accident at the Three Mile Island nuclear power plant in Pennsylvania released an estimated 15 curies of iodine-131.
DOWNWINDER
Downwinder is a commonly used term which refers to people living in the pathway of radioactive releases from a nuclear plant or from atomic bomb test sites.
EFFECTIVE DOSE EQUIVALENT (EDE)
This term is used because a radiation dose to one part of the body does not have the same potential health effect as a dose to another part. The EDE is used to put different types of radiation doses on an equivalent basis in terms of their potential for causing damage.
EQUIVALENT DOSE
This is the measure that indicates the degree of biological damage caused by radiation. Equivalent dose is measured in rems.
EXTERNAL RADIATION EXPOSURE
Radiation exposure from a source outside the body is external radiation exposure. The term refers to radiation, such as gamma rays and X-rays, that can penetrate human skin and thus cause biological damage from outside the body. Gamma rays are photons, or electromagnetic waves, that come from the nucleus of the atom. Gamma rays are uncharged and pass through humans at the speed of light. As gamma rays pass through the body, they may damage cells. Cobalt-60 is a source of gamma radiation.
GENETIC EFFECTS
GENETIC EFFECTS A genetic effect is the result of exposure to substances (such as radiation) that cause damage to the genes of a reproductive cell.
GERM CELLS
Germ cells are reproductive cells - spermatozoa and ova.
HALF-LIFE
This is the amount of time it takes for a radioactive substance to lose one-half of its radioactivity. Iodine-131 has a half-life of eight days. At the end of eight days, half of the iodine-131 atoms have undergone decay and converted to stable xenon-131. Half of the remaining iodine-131 will decay into stable xenon-131 in another eight days, and so on. When an atom decays and becomes stable, it is no longer radioactive. Some radioactive substances decay quickly into non-radioactive materials. Others decay over long periods of time into other radioactive materials which, in turn, undergo radioactive decay. For example, uranium-238 has a half-life of 4.5 billion years and undergoes more than a dozen changes before becoming a stable form of lead.
INTERNAL RADIATION EXPOSURE
Internal radiation exposure occurs when a radioactive substance is taken into the body by eating, drinking, or breathing.
IONIZING RADIATION
The types of radiation capable of removing one or more electrons from atoms they encounter, leaving positively charged particles such as alpha and beta, and non-particulate forms such as X-rays and gamma radiation. Ionizing radiation may damage human cells. Non-ionizing radiation includes visible, ultraviolet, and infrared light, as well as radio waves.
ISOTOPES
Different forms of the same chemical element, which have different numbers of neutrons but the same number of protons in the nucleus of their atoms, are called isotopes. A single element may have many isotopes. For example, stable iodine is iodine-127. Its radioactive isotopes include iodine-129 and iodine-131.
LATENT PERIOD
The time between exposure to radiation and the appearance of a delayed effect is the latent period.
ORGAN DOSE
Among the factors to consider in measuring radiation dose is whether a person received a radiation dose to a single organ or to the whole body. For example, when iodine-131 enters the body, it mainly concentrates in the thyroid gland and gives a dose to this organ.
RAD
A rad is a unit used to measure the absorbed dose, or the amount of energy body tissues absorb. However, equal doses of different types of radiation may not have the same effects on the body. For instance, a dose of alpha particles is more damaging than the same dose of gamma rays or beta particles.
RADIATION DOSE
The amount of radiation, or energy, absorbed by a person is called a dose. Units of dose are used to describe the potential for radiation damage to body tissues.
RADIOISOTOPE
The radioactive isotope of an element that has all the chemical properties of the stable form of the element is a radioisotope. The radioisotope undergoes radioactive decay.
RADIONUCLIDE
An unstable form of an element that can decay and give off radiation is a radionuclide. Radionuclide is the same as radioisotope.
REM
The rem is the unit of radiation accounting for the different effects of different types of radiation. In order to calculate the equivalent dose in rem, absorbed dose must first be established. This number is then multiplied by a radiation weighting factor depending on the type of radiation. For beta particles and gamma rays, the weighting factor is 1. Most of the radioactive material released from Hanford emit beta particles and/or gamma rays, so it is easy to convert directly from rad to rem: 1 rad is equal to 1 rem. Doses from alpha particles and neutrons have larger weighting factors.
SOMATIC EFFECTS
The effects of radiation exposure that result from damage to non-reproductive cells are somatic effects. If the number of cells which suffer somatic effects is great enough, then the damage becomes clinically observable.
SOURCE TERM
Source term refers to the amount and type of radioactive material released into the environment.
WHOLE BODY DOSE
Radiation exposure to gamma rays and X-rays from outside the body can give a radiation dose to the entire body, and each organ receives approximately the same dose. Some internal exposure also gives a whole-body dose. Tritium, for example, is a form of hydrogen. Since hydrogen is part of water molecules which are present throughout the body, tritium delivers a dose to all tissues.
X-RAYS
X-rays are similar to gamma rays but are produced outside the nucleus. Their properties are identical to those of gamma rays.
Click Here to
Search This Site
LINKS
Index
Hanford History and Information about Releases of Radioactive Materials into the Environment: 1944-1972
Overview of Radiation and Known and Potential Health Effects
Health Care: Finding a Provider and Getting Health-Related Records
Coping with Uncertainty and Illness
Maps
Glossary
Potery
Earth Facts
My Family
Web Sites
Psychedeliscope
Q Goo
Java Jukebox
Please Sign My Guestbook
